Podcast: Play in new window | Download
 Hello, this is Dr. Daniel Vinograd. I’m a biological dentist in San Diego, and I’m glad to be here with you today. I would like to talk about the root canal controversy. That’s a topic that has actually created a great deal of confusion.
Hello, this is Dr. Daniel Vinograd. I’m a biological dentist in San Diego, and I’m glad to be here with you today. I would like to talk about the root canal controversy. That’s a topic that has actually created a great deal of confusion.
The History Of The Root Canal
Often, root canal treatment is not an easy topic. It’s not a black and white topic, but let me start by addressing the history of root canal therapy. In first century AD, there was the beginning of surgeons draining teeth that were painful. Record shows the first root canal was in 1756 where Philip Pfaff began filling the canals with gold. I imagine gold was a lot less then that it is today.
In the 1900s, the root canal became a bit more predictable. By the 1950s and 1960s, dentists were getting an apparent 80% success rate with them where people were able to keep them for a period of time. In 1963, endodontics, which is the branch that addresses root canal therapy, was accepted as a branch of dentistry.
Advantages & Disadvantages
Some of the advantages of root canal therapy over the years has been its ability to relieve acute pain. It allows you to keep your own tooth, and it’s avoid other procedures that could be quite invasive and decrease the quality of a person’s life. It also holds the arch integrity so that the teeth don’t collapse into a space.
The disadvantage of root canal treatment is the elimination of the internal blood supply of the tooth, and it becomes subject to infections. The tooth becomes more brittle and requires a crown to maintain its integrity. It may also be systemically challenging to an immuno-compromised patient.
Root Canal Alternatives
So, the question is, as far deciding whether you want to remove a tooth or get a root canal, in my opinion, you have to assess the general health of the patient. A patient that has no other systemic problems and basically has a good, healthy systemic immune system would be a better candidate to get a root canal. I’m going to describe the new generation of biocompatible root canal in a second. Obviously, the opposite would be true of an immuno-compromised patient.
It’s also very important to assess the consequences of removing a tooth. First, of all the tooth has to be removed. If there’s an infection, there should be a lot of cleaning post-extraction done, whether it’s with a burr or with a sharp spoon. It should be cleaned out thoroughly. Then, we have to really think of how to replace the tooth. In some potential root canal cases, no replacement may be necessary. A second molar that did not have any opposing tooth and is not going to create any problems with the arch integrity, in those cases you may not need to replace it at all. Most cases, though, you do need to replace it.
Fixed Bridge vs Root Canal
One of the alternatives to root canal treatment would be a fixed bridge, which is an actual combination of two crowns plus the middle piece that has been extracted that will be replaced. Nowadays, we can actually replace them with the nonmetallic bridges. The disadvantage of a bridge is that you actually the two teeth adjacent to the space, which may or may not be a problem, depending on whether those two teeth were already compromised by large fillings or have crowns already. In that case, it really becomes a no-brainer to place a bridge, and avoid the root canal.
Maryland Bridge vs Root Canal
However, if your teeth are in pretty good shape, and you don’t want to destroy some of the tooth structure, there are other alternatives to root canal therapy. One of them would be a Maryland bridge, which is a very non-invasive type of restoration. It requires a little bit of tooth reduction on the adjacent teeth, but it’s a fraction of the reduction that you would have with a regular bridge. Often, they work quite well. One of the disadvantages is that sometimes those bridges need to be re-cemented as the bond, which is usually quite good, is not as strong as with a regular bridge.
Implant vs Root Canal
The next root canal alternative that you have is to replace the extracted tooth with an implant, whether it is titanium or zirconium. One of the advantages of zirconia is that it does not have any metal. Some of the disadvantages of those zirconia implants as an alternative to a root canal, is that they are large implants that require aggressive bone removal and often additional surgeries in the maxilla when there is sinus proximity. They tend to integrate a little bit less efficiently than their titanium counterparts. Because they are one piece versus the titanium that’s two pieces, you have less flexibility as to the direction of the implant, and often you have to re-prepare those teeth in the mouth to be able to fit a crown over them. These preparations and grinding, sometimes, can cause micro-fractures that could create fractures on the implant, and there’s also issues with fractures on the crowns that are placed over the implants.
The implants that we use in our office are called Bicons, which are titanium, but they are half the size of the regular implants, which become very non-invasive. We don’t have great issues with biocompatability with these kinds of implants unless a patient has a particular reactivity to the titanium itself.
Removal Bridge vs Root Canal
The last way you can replace a tooth is with a removal bridge, which is probably the least costly of all above options, but it does not give a great quality of life to remove partial in-and-out on an ongoing basis.
The Biocompatible Root Canal
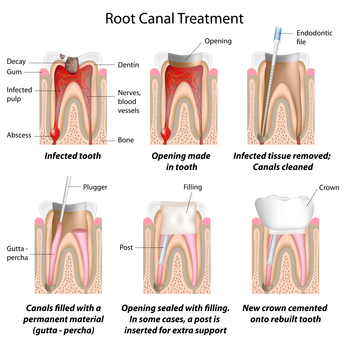
I would not like to address the issue of traditional root canal versus a biocompatible root canal. The traditional root canals have a lot of problems. Mostly, they were filled with gutta percha, which is a rubber, and some type of a sealer. The sealers were actually quite toxic, and the biggest issue with them was they were hydrophobic, which means once they were placed inside of the canal, they tend to withdraw because there’s natural moisture in the environment. That resulted in a lack of seal at the apex, the very end of the root, which became a focus of infection and bacterial growth. Obviously, there were also a lot of accessory canals, small little canals on the side of the tooth, that were not addressed.
With the advent of new materials for root canal therapy, there came a sealer that is actually calcium hydroxide-based that is osteogenic, which means that it stimulates osteoblastic activity, bone formation. Most importantly, it’s hydrophilic; it likes moisture so it takes bit of moisture from its environment and actually swells a little bit. That means that this material, by swelling, can end up sealing not only the main canal but also the accessory canals as well.
Another great advantage of this material that we use in our office is called Bee Sealer, is that it has a pH of 12.8, and it really doesn’t solidify for 24 to 48 hours, which means that you have a material that is sterilizing that canal and the accessory canals for that period and beyond (but the most active sterilization at pH12.8 happens during the first 24 to 48 hours).
Now, the American Society of Microbiology published an article by Mendonca, Amaroso, and Knabel. It in, it speaks about the research that at pH 12, the pathogenic bacteria are destroyed. The cytoplasmic membrane of the bacteria disintegrates. So, a pH of 12.8 would be incredibly efficient in sterilizing the canal.
Bottom Line, Should I Have a Root Canal?
Now, is root canal therapy for everyone, even the biocompatible one? I would say no. Again, you have to pay attention to the condition of the patient or your condition. Quite obviously, if you are immunocompromised or you’re dealing with some serious systemic disease, you may want to opt for not having this done. However, you really should consider a lot of the options post-extraction that you have to face, and may your decision before and not after the extraction.
I hope this is helpful. All the best. Dr. Daniel Vinograd, again. Take care.
A Message From Dr. Vinograd & His Patients
To make an appointment with Dr. Daniel Vinograd for a Free Consultation, please call


 Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here:
Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here: 

[…] See Dr. Vinograd’s remarks next week here: Root Canals (commentary) & Podcast on the subject Episode 3: Root Canal. […]
[…] my patients decide to extract a tooth that is infected or has existing root canal I provide the following information about their […]