The Best Toothpaste Is A Fluoride-Free Toothpaste You Make Yourself
So What Is The Best Toothpaste?

That’s an important question, but before we talk about the best toothpaste — that is the right fluoride-free toothpaste that doesn’t have any dangerous, toxic ingredients — there are other things that are just as concerning to me about overall health. Once we’ve addressed those, I’ll tell you my ideas about toothpastes and how to make your own toothpaste to use every day.
My biggest concern is with the big picture — the overall health of people like you and the things you do to sabotage your health, including consuming unhealthy foods and using unhealthy products that contain additives and chemicals and expose you to toxins on a regular basis. Soaps, detergents and even the air we breath all contain chemicals we should find ways to avoid.
But now, let’s talk about the best toothpaste for you and your needs.
Choosing The Best Toothpaste Or Using Homemade Toothpaste
Even a fluoride-free toothpaste that is promoted as safe and natural contains potentially harmful chemicals. These chemicals can be absorbed by the permeable oral mucosa and into our systems. Some of the most concerning ingredients are:
- Triclosan, which can be contaminated with dioxin, a pesticide that causes strong hormonal disturbances.
- BHT, an allergen that can cause immunologic and reproductive problems.
- Fluoride, which has developmental and reproductive toxicity.
- PEG-12, which is toxic and may be contaminated with ethylene oxide.
- FD&C Blue, which can bioaccumulate and become toxic.
- Sodium hydroxide, which is toxic to organs.
- DEA, a foaming agent that can cause cancer and disrupt hormones.
- Propylene glycol, a primary ingredient in antifreeze that the EPA requires workers to handle with gloves and is quickly absorbed by the mucosa in the mouth.
The best toothpaste also does not contain sorbitol, sodium lauryl sulfate, sodium saccharin, carrageean or manganese gluconate.
While few toothpastes on the market are perfect, the following brands market themselves as natural, and many of them also offer flouride-free toothpaste choices:
- Auromere Ayurvedic Herbal
- Desert Essence
- Dr Ken’s
- Jasons
- Kiss My Face
- Nature’s Gate
- Spry
- Tea Tree Therapy
- Tom’s of Maine (owned by Colgate)
- The Natural Dentist
- Vicco
- Weleda
Make Your Own Great-Tasting Fluoride-Free Toothpaste
Some of the brands above taste terrible, and some still contain objectionable ingredients. For the best possible toothpaste solution, consider making your own homemade toothpaste. Here is my not-so-secret-anymore recipe for great-tasting, highly effective and completely safe toothpaste:
- ½ cup of non-hydrogenised virgin coconut oil
- 2 to 3 tablespoons baking soda OR 1 tablespoon fine pumice
- Xylitol, a sweetener, to taste
- 12 to 20 drops cinnamon or peppermint essential oil (or any other flavor you like)
To create the toothpaste, soften the coconut oil slowly over gentle heat, then add other ingredients and mix well. Cool completely before use, and store in a glass jar.
This healthy toothpaste isn’t just safer than what you’re using now, it can be made at a fraction of the cost too.
It’s Worth It For Good Health
Making your own toothpaste is worth the effort to avoid sodium lauryl sulfate or SLS. This common ingredient in soaps, shampoos and lotions is found in most toothpastes and functions as a surfactant. Some people have no immediate reaction to it, but others are allergic. It has also been linked to canker sore flare-ups and dry mouth. It can even temporarily alter taste, ruining your next meal.
Studies on SLS are inconclusive, but many researchers have indicated concern with its use. That means it may be safest to use an SLS-free toothpaste. A Harvard study has even endorsed use of safer toothpastes.
A healthy oral environment can also reduce the risk of serious disease, including stroke, respiratory disorders, heart disease and even problems during pregnancy. While a toothpaste labeled as natural may be good enough, a natural, homemade toothpaste can be even better. The best toothpaste formula like the one above contains nothing that’s harmful or questionable.
In addition, keeping your mouth healthy is almost impossible if its pH level is wrong. For the healthiest possible mouth, you need to neutralize the overall pH of your mouth. That keeps acid from being able to destroy tooth structures, and it helps keep plaque from forming too. Since plaque contains bacteria that can be harmful to your teeth and your health, it makes sense to eliminate it.
Bacteria love acid, and acid directly destroys too, so neutralizing it is an intelligent idea. Saliva helps with pH balance, and using my homemade best toothpaste recipe helps even more.
Would you like to learn more about the best toothpaste possible and make sure your oral health is as it should be? Contact natural dentist Dr. Daniel Vinograd at [email protected] or (619) 630-7174.
Root Canal: The Controversy (Podcast)
Podcast: Play in new window | Download
 Hello, this is Dr. Daniel Vinograd. I’m a biological dentist in San Diego, and I’m glad to be here with you today. I would like to talk about the root canal controversy. That’s a topic that has actually created a great deal of confusion.
Hello, this is Dr. Daniel Vinograd. I’m a biological dentist in San Diego, and I’m glad to be here with you today. I would like to talk about the root canal controversy. That’s a topic that has actually created a great deal of confusion.
The History Of The Root Canal
Often, root canal treatment is not an easy topic. It’s not a black and white topic, but let me start by addressing the history of root canal therapy. In first century AD, there was the beginning of surgeons draining teeth that were painful. Record shows the first root canal was in 1756 where Philip Pfaff began filling the canals with gold. I imagine gold was a lot less then that it is today.
In the 1900s, the root canal became a bit more predictable. By the 1950s and 1960s, dentists were getting an apparent 80% success rate with them where people were able to keep them for a period of time. In 1963, endodontics, which is the branch that addresses root canal therapy, was accepted as a branch of dentistry.
Advantages & Disadvantages
Some of the advantages of root canal therapy over the years has been its ability to relieve acute pain. It allows you to keep your own tooth, and it’s avoid other procedures that could be quite invasive and decrease the quality of a person’s life. It also holds the arch integrity so that the teeth don’t collapse into a space.
The disadvantage of root canal treatment is the elimination of the internal blood supply of the tooth, and it becomes subject to infections. The tooth becomes more brittle and requires a crown to maintain its integrity. It may also be systemically challenging to an immuno-compromised patient.
Root Canal Alternatives
So, the question is, as far deciding whether you want to remove a tooth or get a root canal, in my opinion, you have to assess the general health of the patient. A patient that has no other systemic problems and basically has a good, healthy systemic immune system would be a better candidate to get a root canal. I’m going to describe the new generation of biocompatible root canal in a second. Obviously, the opposite would be true of an immuno-compromised patient.
It’s also very important to assess the consequences of removing a tooth. First, of all the tooth has to be removed. If there’s an infection, there should be a lot of cleaning post-extraction done, whether it’s with a burr or with a sharp spoon. It should be cleaned out thoroughly. Then, we have to really think of how to replace the tooth. In some potential root canal cases, no replacement may be necessary. A second molar that did not have any opposing tooth and is not going to create any problems with the arch integrity, in those cases you may not need to replace it at all. Most cases, though, you do need to replace it.
Fixed Bridge vs Root Canal
One of the alternatives to root canal treatment would be a fixed bridge, which is an actual combination of two crowns plus the middle piece that has been extracted that will be replaced. Nowadays, we can actually replace them with the nonmetallic bridges. The disadvantage of a bridge is that you actually the two teeth adjacent to the space, which may or may not be a problem, depending on whether those two teeth were already compromised by large fillings or have crowns already. In that case, it really becomes a no-brainer to place a bridge, and avoid the root canal.
Maryland Bridge vs Root Canal
However, if your teeth are in pretty good shape, and you don’t want to destroy some of the tooth structure, there are other alternatives to root canal therapy. One of them would be a Maryland bridge, which is a very non-invasive type of restoration. It requires a little bit of tooth reduction on the adjacent teeth, but it’s a fraction of the reduction that you would have with a regular bridge. Often, they work quite well. One of the disadvantages is that sometimes those bridges need to be re-cemented as the bond, which is usually quite good, is not as strong as with a regular bridge.
Implant vs Root Canal
The next root canal alternative that you have is to replace the extracted tooth with an implant, whether it is titanium or zirconium. One of the advantages of zirconia is that it does not have any metal. Some of the disadvantages of those zirconia implants as an alternative to a root canal, is that they are large implants that require aggressive bone removal and often additional surgeries in the maxilla when there is sinus proximity. They tend to integrate a little bit less efficiently than their titanium counterparts. Because they are one piece versus the titanium that’s two pieces, you have less flexibility as to the direction of the implant, and often you have to re-prepare those teeth in the mouth to be able to fit a crown over them. These preparations and grinding, sometimes, can cause micro-fractures that could create fractures on the implant, and there’s also issues with fractures on the crowns that are placed over the implants.
The implants that we use in our office are called Bicons, which are titanium, but they are half the size of the regular implants, which become very non-invasive. We don’t have great issues with biocompatability with these kinds of implants unless a patient has a particular reactivity to the titanium itself.
Removal Bridge vs Root Canal
The last way you can replace a tooth is with a removal bridge, which is probably the least costly of all above options, but it does not give a great quality of life to remove partial in-and-out on an ongoing basis.
The Biocompatible Root Canal
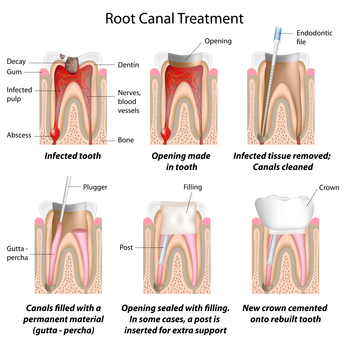
I would not like to address the issue of traditional root canal versus a biocompatible root canal. The traditional root canals have a lot of problems. Mostly, they were filled with gutta percha, which is a rubber, and some type of a sealer. The sealers were actually quite toxic, and the biggest issue with them was they were hydrophobic, which means once they were placed inside of the canal, they tend to withdraw because there’s natural moisture in the environment. That resulted in a lack of seal at the apex, the very end of the root, which became a focus of infection and bacterial growth. Obviously, there were also a lot of accessory canals, small little canals on the side of the tooth, that were not addressed.
With the advent of new materials for root canal therapy, there came a sealer that is actually calcium hydroxide-based that is osteogenic, which means that it stimulates osteoblastic activity, bone formation. Most importantly, it’s hydrophilic; it likes moisture so it takes bit of moisture from its environment and actually swells a little bit. That means that this material, by swelling, can end up sealing not only the main canal but also the accessory canals as well.
Another great advantage of this material that we use in our office is called Bee Sealer, is that it has a pH of 12.8, and it really doesn’t solidify for 24 to 48 hours, which means that you have a material that is sterilizing that canal and the accessory canals for that period and beyond (but the most active sterilization at pH12.8 happens during the first 24 to 48 hours).
Now, the American Society of Microbiology published an article by Mendonca, Amaroso, and Knabel. It in, it speaks about the research that at pH 12, the pathogenic bacteria are destroyed. The cytoplasmic membrane of the bacteria disintegrates. So, a pH of 12.8 would be incredibly efficient in sterilizing the canal.
Bottom Line, Should I Have a Root Canal?
Now, is root canal therapy for everyone, even the biocompatible one? I would say no. Again, you have to pay attention to the condition of the patient or your condition. Quite obviously, if you are immunocompromised or you’re dealing with some serious systemic disease, you may want to opt for not having this done. However, you really should consider a lot of the options post-extraction that you have to face, and may your decision before and not after the extraction.
I hope this is helpful. All the best. Dr. Daniel Vinograd, again. Take care.
A Message From Dr. Vinograd & His Patients
To make an appointment with Dr. Daniel Vinograd for a Free Consultation, please call
Transcribed P4: June 2013: Holistic Dentistry & Biocompatible Protocols (Lecture to Gerson Institute)
Right. Actually, I’m in San Diego, often there are people that don’t have insurance and have a hard time affording, and that is a big question. There is a big problem. I used to have a friend who went to USC with me and opened a practice in Tijuana, and I used to send all those patients to him. I have not seen a lot of really, really great work coming back from Tijuana, although I’m sure there’ some really great people. If you have a really good dentist, please let me know because I’m sure they’re there. I just haven’t found it. So, I couldn’t recommend anybody there. The costs are much less there. The cost of labor is less and insurance and things like that. So, they are able to keep the prices lower.
If you don’t find somebody like that, I would suggest that you compromise. First of all, it’s what we do for our patients is we do a treatment plan. This is where you are right now. This is where I want you to be, where you want to be, in perfect health. Here-to-here, sometimes there’s a little path to go. Sometimes, there’s a huge cast. So, we try to take priorities and start slowly, going a bit at a time, making sure that we’re moving forward.
Aside from that, you have choices to make, and you can replace, for example, with composite materials, or you can replace them with porcelain. Porcelain would be preferable. It’s a much more biocompatible mixture. However, if there are issues with finances, sometimes you can replace them with a good composite material. I think every composite material that I know in the market has BPAs with at exception of one that I think is called beauty fill. That’s the one we use in our office. It has no BPAs. Having said that, I will really encourage people who have very large amalgams not to use that because those materials will break down and erode. When you have smaller restorations, then it’s not a problem. You can use composite very successfully, and we do that, too. We try to be conscientious about people’s financial struggles, too, but that’s a reality. Thanks for bringing that up.
Hello. To take out the traditional root canal or do these replacement with this biocompatible materials, is it a big thing to take out the roots or is it a better thing to fill them with these biological things. I don’t know.
I’m not sure I understand your question but let’s work with this. So, in a root canal, we’re basically. Let me see if I can go back far enough. So, you understand that root canal, they actually just take out the inside here. The tooth stays in place, everything stays in place. They are only taking out this little material here, which is like a little bit of tissue. So, in traditional root canal, they remove this. They enlarge this area a little bit, and then they fill it with material. Now, that’s a root canal.
A biocompatible root canal is, the only different between the two, is a biocompatible material is used to fill this area right here.
But how do you take that out?
Now, a lot of patients come over to try to change old root canals for a new root canal, a biocompatible root canal. Then we decide whether we just want to take the tooth out or if we want to retreat this with biocompatible materials. So, a lot of the times, dentists put very large metal posts to reconstruct the tooth into this canal. When that happens, there’s no way to retreat the tooth, and the tooth needs to be extracted if it’s becoming a problem. If it doesn’t have a large post, and I would say 30% we cannot retreat then and 70% of the team we can retreat them. So, what we do is we have special computerized machinery that they’re rotary files. We go in there, and we actually remove all the material. The tooth still stays in place. Nothing happened to the tooth. It’s only the inside, it’s like a tunnel inside that gets worked on. So, we would go in here and remove all the old toxic material and refill it with a biocompatible material.
Which is not toxic at all?
It’s not toxic. It’s calcium hydroxide-based, and they use that a lot in hip replacements, knee replacements to generate bone. So, if you take this material and place it on the bone, the bone will grow on it quite happily.
Dr. Vinograd, I have one from the live stream. Does rinsing with hydrogen peroxide prevent most gum infections? Some dentists believe it introduces free radicals and may be toxic to rinse with.
Yes. I agree. I don’t think it’s the best solution. It will kill bacteria, and some people will use it, sometimes use 50-50 with water. Some people will use bacteria, but having an option of doing that or ozone, which is pure oxygen, is a no-brainer. Why would you want to use anything that’s irritating and creates free radicals. It will do the job and clean the bacteria, number one, and number two, it will only reach bacteria on the surface if you are rinsing. It’s not really going to help you that much unless you’re water pick with that to really deliver the material deeply into the gums.
So, we have two issues. One is the delivery system. We want to have a delivery system to get to the bottom of the pocket, and second, we want the most biocompatible, clean type of substance that will kill the bacteria. Ozone therapy has been proven to be much more effect than even antibiotic therapy in killing anaerobic bacteria inside the pockets without any side effects. You’re basically introducing oxygen-concentrated water.
How do you remove cavitations when having teeth removed such as wisdom teeth?
Well, cavitations has a lot of different definitions for different people. We don’t use the word cavitations anymore because of its legal implications. There have been dentists that have been sued because they were claiming they were doing cavitations. I will addesss mostly what the concern is, which is when a tooth gets infected, the bone around it gets infected. Sometimes when doctors extract a tooth and don’t really go back in there and scrape that infected bone, it often, especially in wisdom teeth, not only do you have an infected bone, but you also have a little sac that was actually engulfing the tooth as it was coming out. Sometimes that creates a great cyst in the area. So, you have to get in there and get that little sac out as well as any infected bone around it. You just want to have a dentist that will be conscientious and really go in there and clean anything that is infected around the tooth. For example, if you have a tooth that is extracted for orthodontic reasons, really, there is not issue. The issue is when you have an infection in the tooth that’s actually moved into the bone tissue.
I have two questions Doctor. One on root canal. Do you have to be an endodontist to do that?
I’m not an endodontist. I probably do 5 or 6 root canals a week. So, you don’t need to be. There are times when you want an endodontist to do it. I don’t refer my patients to endodontists because I have a friend in San Diego who’s using the biocompatible materials, and nowadays, we have computerized systems.
It’s not what it used to be. Endodontics used to be quite complicated before. We use a rotary system that’s connected to a computer, and I go in there. It tells me when I’ve reached the tip here. It autoreverses. My partner calls it Root Canal for Dummies. So, it’s become a lot less complicated to do a root canal. We usually do a root canal for an hour from beginning to end. Shorter time. Yeah. We have better materials, better instruments, and so forth. Having said that, there might be some cases that are complicated enough that might be referred to the endodontist, and the dentist himself needs to feel comfortable with the endodontic procedure. So, it varies from person to person.
Another question, sir. You mentioned about using the water pick and the mouth wash.
It’s not actually a mouth wash.
No, no I know, I’m talking about mouthwash. When you put the water in the water container, is it advisable to put the mouthwash in there or do the mouth wash after?
No mouthwash at all. The only thing I’m advocating is using an ozone generating machine. You have a little tube. It has a head on it. You put it on the container with the regular water, purified water hopefully, and you let it sit there for 15 minutes, and that becomes your super mouthwash.
Thank you.
We have another one Dr. Vinograd, from the chat room. This is Mary, and she’s looking at you from this camera and she’s asking, are there any problems biologically with the materials traditionally used in dentures?
Yes. For a susceptible person, you really must be quite careful in the materials that you use. Materials have advanced quite a bit. They’ve become less toxic. There are now flexible partials that are being used that are quite benign and also easy to use. So, yeah. You want to make sure that you are using materials that are from the last generation of dental materials versus the old materials that had quite a bit of toxins and heavy metals.
I would like to ask you, what do you think about removing bacteria by oil, that’s my first question, and the second question, whether you recommend or don’t recommend the mouthwash at all, what it does, what’s good on it, and not good.
Okay. What’s good in it is that you make a lot of stockholders very wealthy and also gives you a nice fresh feeling, and then you can join the commercials and jump around with the people who are jumping around in the commercials with good breath. It does give you a good breath for a very short period of time, and the alcohol kills some bacteria. What’s bad about it is that it has a lot of alcohol, dehydrates the tissues. It’s just really not good, and they’re chemically loaded so, I would not use mouthwash at all.
Natural? If you want to use ozonated water as a mouthwash, that will work better and longer than a mouthwash. It doesn’t give you your initial, oh my god I taste like mint or I smell like mint, but it would really be effective. There’s two reasons, most of the time, why you have bad breath. One, it’s going to be dental issues, gum disease, particularly, or GI tract problems. If it’s GI tract problems, no matter what you do to your mouth, it’s not going to solve it because it’s coming from deep inside. If it’s a problem with your mouth, your gums, inflammation, the ozonated water will work much, much better than any commercial mouthwash.
The first part of your question?
Oil pulling.
Oil pulling. There’s a lot of research on oil pulling, a lot of information right there. I feel that it’s a very valid protocol, and a lot of my patients use it, but again, you are going to be much more effective with the ozone if your purpose is to kill bacteria. Much more effective. Remember again, the anaerobic bacteria are the ones that cause most of the damage in the mouth, both in caries and in your gum disease, and those are the ones that are going to be killed by the ozone.
Question for you. I recently visited my dentist, and we had a discussion about mercury fillings. I said I want to take them all out, and he advised against that because he thought that the ones I had, he had taken one out and put a crown in. The other ones didn’t show any leakage and looked good. I just wanted your opinion on that. Would you leave them in, or would you have them out?
You know, in my book, the only good amalgam is dead amalgam. Eventually, those amalgams are going to cause you trouble so the question is do you want to take a chance, play Russian roulette, whether to decide what to do in the long run, he was right or he was right? Maybe he’s right. They’re causing no problems. It could be 100 years from now, 200 years from now, maybe we’ll have the answer, but why would you want to keep something in there that is 50% mercury, third most toxic material that we know, and that eventually is going to end up cracking your teeth?
Isn’t it better to really remove them now before physical damage takes place? When you still have the question mark, in my book there’s really no question. I would not keep a single amalgam in my mouth. So, a lot of the larger amalgams would inevitably, I am putting money on the table right now, that they will crack in time, sooner or later. So, it really is a no brainer.
For some of us that don’t have the ozone water right now, would you recommend the acidic water versus the alkaline water to rinse your mouth that way?
That’s not going to make a lot of difference. Having said that, there are a lot of people that have slightly higher pH than others. If your pH is slightly higher, you will know that because you tend to build up a lot of tartar on your gums and have very little problem with decay. On the other hand, if you have very acidic saliva, you will tend to have a lot more decay and very little tartar. Those are the two extremes. Of course, there are people in between.
If you have a very alkaline saliva where you’re building a lot of tartar in your gums, I would use probably use water with a slight lemon in it or anything that will acidify it or perhaps some apple cider vinegar, just a little bit, just to bring the pH down a little bit so you don’t have the issues with the tartar formation. If you, on the other hand, you have slightly more acidic, and you’re having a lot of problems with decay, there are two things you could do. One is put a little baking soda in the water to rinse. The other thing you could do is use xylitol chewing gum that’s really been proven to decrease decay and is fairly a natural sugar. My son uses it. I wouldn’t have any hesitation using that. Having said that, most of us can get an ozone generator, a couple hundred dollars on the internet.
Okay I think we’re going to try to sneak in one more.
Okay.
Doctor. For a younger kid who has a hypothyroidism, has amalgam on some of the temporary teeth, the baby teeth.
How old is the child?
Nine. What do you recommend? Just to wait it out?
Nine years old. By 11 years old, he’s going to shed most if not all of his baby teeth. So, being nine years old and having had the amalgams for a long time. He had those amalgam fillings for a long time?
Yes.
If he came to my practice, and he’s nine. If he had fairly normal patterns as far as the timing of the teeth coming out, I would probably not take them out. I would let them come out on their own because in a very short period of time, he’s going to have them out. If the amalgams are not being taken out properly, it’s going to do more damage than good. So, at nine, I would probably wait it out.
Well that’s going to about do it, but I think we all appreciate you coming to us today. Let’s all give Dr. VInograd a big hand.
Thank you, and I want to thank the Gerson Institute. They do an awesome job, and I’m proud to be associated with you guys.
We’re going to include, in the e-mail package that we send to you next week when we get around to it or when it’s all compiled, we’re going to include Dr. Vinograd’s powerpoint presentation so you will have all that also. He just agreed to do it. Yay!
If you guys just want to take a couple more minutes to finish filling out your evaluations, and when we leave, we’re going to put them out in the holder that’s out there in the hall. I just want to take a moment to tell you how honored we were to have all of you here this weekend. It was absolutely fantastic. We were so excited that you came, and everyone at the Institute is grateful for your participation in all of this. I also wanted to let you know that you may be leaving here this weekend with a mental illness, and I’m not making this up. Right now, the psychiatric community is debating whether or not to include a new diagnosis called orthorexia into their diagnostic and statistical manual.
They’re writing papers about it. They’re trying to gin up a lot of enthusiasm about this, and what orthorexia actually is, by their definition, is an unhealthy fixation on clean and healthy food. It is an offset of anorexia, which is people who don’t eat anything, and they’re claiming that this can potentially become a diagnosable mental illness for which they can prescribe psychiatric mediation. I don’t know about the rest of you, but I am perfectly happy to spend the rest of my days in the looney bin with the rest of you toasting each other with glasses of carrot juice.
Thank you all so much. Be well, stay bold, and safe home
Now Accepting: Geha Dental | Metlife | Cigna | Delta Dental Insurance
We are happy to help you achieve your goals in a warm environment; with safe, non-toxic materials.
SKIP TO YOUR INSURANCE: Geha | Metlife | Cigna | Delta | Guardian | Aetna | Humana
Geha Dental Insurance Accepted

San Diego Dentist (centrally located in the San Diego area) is now accepting Geha Dental Insurance as well. Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Geha dental patients can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Geha Dental Coverage information to get started.
Metlife Dental Insurance Accepted

San Diego Dentist (centrally located in the San Diego area) is now accepting Metlife Dental Insurance. Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Metlife dental patients can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Metlife Dental Coverage information to get started.
Cigna Dental Insurance Accepted

We are also now proud to accept Cigna dental insurance at our new facility, San Diego Dentist (centrally located in the San Diego area). Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Cigna dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Cigna Dental Coverage information to get started.
Delta Dental Insurance Accepted
 We are now proud to accept Delta dental insurance at our new facility, San Diego Dentist (centrally located in the San Diego area). Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Delta dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Delta Dental Coverage information to get started.
We are now proud to accept Delta dental insurance at our new facility, San Diego Dentist (centrally located in the San Diego area). Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Delta dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Delta Dental Coverage information to get started.Guardian Dental Insurance Accepted

We are now proud to accept Guardian dental insurance at our new facility, San Diego Dentist (centrally located in the San Diego area). Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Guardian dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Guardian Dental Coverage information to get started.
Aetna Dental Insurance Accepted

We are now proud to accept Aetna dental insurance at our new facility, San Diego Dentist (centrally located in the San Diego area). Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Aetna dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Aetna Dental Coverage information to get started.
Humana Dental Insurance Accepted

San Diego Dentist (centrally located in the San Diego area) is now accepting Humana Insurance as well. Dr Vinograd offers general, family, and cosmetic dentistry for all ages – with a focus on the doctor-patient relationship, and patient comfort. Humana dental carriers can rest assured that the latest (and even some proprietary) methods will be employed to promote comfort, trust, and assuage pain. Call (619) 630-7174 with your Humana Dental Coverage information to get started.
About Doctor Vinograd
“I am quite conscious that dentistry has to be embraced side by side with the systemic health and emotional wellbeing of my patients. That is why I place such high value on the relationships with those who entrust me with their health. I feel blessed to go to work every day to do something I love, creating special connections while contributing to the wellbeing of others. I understand that most of us fear pain as a result of past dental experiences. The foundation of doctor-patient relationships in my practice is based on earning you trust. I am committed to dental excellence and painless dentistry.” – Dr. Daniel Vinograd, DDS.
*Don’t see your insurance? Call (619) 630-7174, we would be happy to look into your coverage with you.
Partial List of Accepted Insurance: Guardian dental insurance, Geha dental insurance, Aetna dental insurance, Humana dental insurance, Guardian Life dental insurance, Guardian Anytime dental insurance, Guardian insurance, Geha insurance, Aetna insurance, Humana insurance, Metlife dental, Cigna dental, Delta dental, Metlife dental insurance, Cigna dental insurance, Delta dental insurance, Geha dental.
Transcribed P3: June 2013: Holistic Dentistry & Biocompatible Protocols (Lecture to Gerson Institute)
Of course, you don’t want to continue to have that bacterial count in there, but there was one particular patient, a dear, dear patient of mine. Her name is Judy, and she said, “Doc. I just don’t want to get rid of my teeth.” Her teeth are dangling, big pus pockets, 7, 8, 10 millimeter pockets, and she says, “Doc. There’s no conversation here. I’m not doing anything about this.” I said, “Judy we need to talk about the biological component of this.” So, we got here to get a water pick.
This was many, many years ago, but Judy’s the one individual that really motivated me to develop this technique. Then, we got her to stop by using the water pick. When she started using the water pick and got proficient with it, which sometimes takes a week or two to get proficient with it, we added and ozone machine. I’m sure many of you are familiar with ozone. Many dentists used ozone. My feeling is that ozone is a little bit irritating when it’s in the air, but once you get it in water, it’s very safe.
Ozone, O3, we’re supercharging the water with oxygen. So, if we can actually deliver that oxygenated water into those deep pockets, what’s happening to the bacteria? They’re doing on contact. They hate it. So, the ozone, we know, will kill anaerobic bacteria. We know that, but how do we deliver it to 7, 8 millimeter pockets? We use a water pick.
Suddenly, ozone machines used to be a couple thousand dollars. They’re no longer that. They’re much, much less than that today. Now, we’ve gotten a lot of our patients on this protocol, the ozonizer with the water pick, and by the way, Judy still has her teeth. The 10 millimeter pockets became 8 millimeter, and the 6 millimeter became 4s. There’s improvement, but 8 millimeter pockets are still not a good place to be. She could go every day and clean them out. So, those bacteria that could possibly travel into your system are no longer a challenge for her.
A lot of people asked me last time I was here, where do I get these ozone generators and so forth. So. I’m going to tell you generally what you want. You want to use them in a well-ventilated area, first of all. Then, you want one that is a Corona discharge. This is the kind of machine that if you used to do it, I want you to look for. You want 1000 milligrams per hour, which is a powerful machine enough that you don’t have to sit for three hours ozonizing your water. This will probably do it in 15 minutes, and then you want a sealed box around the elements because there are a lot of people making them at home now. I do not recommend that you actually get a home-made unit. You need to get one that’s well-sealed in a box.
Now, this is actually my son’s company, and I asked him to source the machine that I wanted. If you don’t find it anywhere else, you can always find it with him. I’m not promoting that you get it from him. If you get it cheaper everywhere else, it’s fine, but I asked him to get the machine that I wanted in his website. You could always get it there if you find it nowhere else.
Now, what about the water irrigation device, the water pick. You want to get as inexpensive a device as you can get. It really doesn’t matter. What you need to get is one that has a container because they have some that are just individuals. You don’t want that, the travel kind. You can’t get enough water in there, but anything that has some kind of reservoir where you put water and use that water for the water pick is good. You can get it fairly inexpensive now at any of those big box stores.
You want to use the middle pressure. You don’t want to go to the high pressure when you do this because you can actually start creating more of a deepening of the pocket with the pressure. So, medium’s enough to reach the bottom of the pocket, and you don’t have to have gum disease. Two to three millimeter pockets are also quite receptive to getting cleansed with our irrigation device.
Lastly, this is great thing to do, but you still want to go every six months to get your gums checked. If your dentist is not checking your gums every time that you go for a checkup, you need to switch. You need to find somebody who will be very conscientious of your gums and of gum disease because that’s really one of the biggest challenges for your health.
Okay. This is another big, big questions. For me, it’s been one of the challenging issues in my practice. This is the root canal controversy. Who in this group has hear that root canal is not good for you? Okay. What do you do when a tooth is killing you, you’re in terrible pain, you go to the dentist, he says you need a root canal. It’s a first molar, and you have to decide. What do I do? Do I do a root canal? Do I extract this tooth? If I extract this tooth, how is that going to impact my chewing ability, my quality of life? If I extract it, do I replace it? Do I not replace it? This is a challenging question, both for the dentist and for the patient.
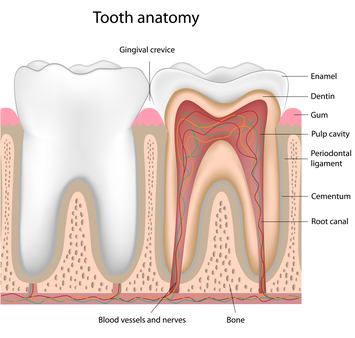
So, these are some of the choices that we have to make. Now, what is happening when somebody needs a root canal? In most cases, we have a tooth. Inside of here, we have a vein, an artery, and a nerve in a package going on the inside of the tooth. Usually when we need a root canal is when we’ve had a breakage on the integrity of the tooth, the white part, that has given the ability to bacteria to introduce themselves into the canal where there’s a lot of blood supply, a lot of nourishment for them. So, it creates great inflammation.
As you can see, if you get a tummy ache, and it starts hurting you, you get the distended stomach. It just awful, the pressure and the pain. In the tooth, if you get that area inflamed, there’s no place to go. It’s against hard structures. That’s why toothaches are so terrible. They’re so difficult to manage.
So, what are the options to replace extracted teeth? Well the first question is, do we extract it or do we do a root canal? Now, a root canal, traditionally, a dentist will come in and remove all this tissue, which is soft tissue, infected tissue, and will actually fill this canal up to here optimally with a material. Some of the objections to root canals in the past, number one is that you no longer have that blood supply from the inside of the tooth. Is that the only blood supply to the tooth? No, you also get blood supply from around the tooth, but yes, if you have a root canal, the tooth becomes a little bit more dehydrated, more brittle with less blood supply. The biggest issue is not so much that.
The biggest issue is that the filling materials that have been used in the past have been number one, been hydrophobic, which means they hate moisture, and there’s always going to be moisture.
So, they actually contract and create spaces between the material and the tooth. The second problem is that they’ve been incredibly toxic. The materials used in root canals have been incredible toxic in the past. So, I, for many years, stopped doing root canals.
I began seven, eight years ago with the advent of new materials where we make a decision based on the individual. If you are a strong individual, not immune compromised, not dealing with a severe illness, I would consider doing a biocompatible root canal where I would fill those root canals with a biocompatible material that’s hydrophilic, expands, and seals the material really well, not giving place to those gaps that we had before where the bacteria used to get in there and colonize.
If I have somebody that’s immune compromised, somebody who’s dealing with a severe challenge with their health, then we have to look at the big picture. We don’t want to keep a possible focus of infection in the mouth when you’re dealing with such a severe issue. So, again, trust yourself. Trust the people that you’re around to make good decisions. Look at the big picture. Don’t just go with that you read in the internet. So, I’m giving you information here so you can actually make good decisions together with your health professional.
Once we’ve decided to extract the tooth, what do we do? Implants? Fixed bridges? Removable bridges? Maryland bridges? Those are the four most common options that we consider in our practice. Implant. Advantage of the implant, they’re solid, they integrate really well to the teeth right now. They have about a 97% success rate. Some of the challenges with the implants. First of all, they’re made out of metal. Do you want metal in your bone if you’re dealing with big issues and allergies and metal problems in your mouth? If you’re immune compromised, I would not suggest that you get that. If you’re healthy and this is an important tooth to replace and you have no major issues, that’s a possibility. Some of the problems in the past was that there was leaking in here, right between the implant in the tissue where there was leakage and bacterial infection.
Nowadays, the designs of the implants have improved where that’s become less of a problem, but again, decision time. Don’t just think it’s always this way or always that way. Use the information that you have to make good decisions.
Removable bridges. Probably, they’re very, very noninvasive. You are basically placing something in there as long as you have relatively good biocompatible materials, but they’re not necessarily the best for your quality of life. It’s something that you have to put on and off all the time, and as people who have them will tell you, some people adjust really well to them. Some don’t, and they usually end up in the drawer with all the other gadgets that they bought and they can’t use.
Fixed bridge. We would actually take two teeth on the side. We would reduce them, and then we would actually place a bridge in there. Nowadays, we’ve actually gotten to the point where we can actually do bridges without any metal whatsoever. Biocompatible bridges. New material called bruxor that is as hard as they come is actually not a hybrid material. It’s very biocompatible, and you can take a hammer to that material and try to break it. You can’t. The disadvantages are that you may sometimes have two pristine teeth on the side. You don’t want to grind those teeth, but if you have two crowns already there, it’s a no brainer. Again, use the information to make good decisions.
Lastly, a Maryland bridge, where if you sometimes have certain parts of the mouth where you can get enough retention. You don’t have enough 300-pound wrestler that’s going to put a lot of pressure on every bite, sometimes we can actually get away with not having to grind the whole tooth and just doing a partial design and just do a Maryland bridge. It used to be en vogue 30 years ago. Then, people stopped using them. Now, with the advent of better bonding materials, we’re able to come up with those types of designs successfully.
That’s basically what you have to do. Instead of preparing the whole crown, you just have to remove much lesser amount of enamel of the tooth to get that bridge. Now, what materials can you use in crowns and bridges? Porcelain to metal, and the metals are non-precious, semi-precious, and precious. No matter what metal you’re using, unless you’re using pure titanium, they’re all different amalgamated metals. Not to be confused with metals. There is really no mercury there, but a lot of them have platinum, nickel, so forth. Then you have no metal crowns. Some, lava, emax, and empress, that are bi-layered, which means you have a core and a beautiful overlay of porcelain. Then you have the pure zirconia. The pure zirconia is, by far, the most biocompatible material and the best crown from the health point of view.
However, sometimes we don’t use them in the front because they’re not quite as beautiful as the bi-layered. So, again, if you don’t really want to have a dead-looking bridge or some crowns in front, then you may want to choose to go bi-layered. If it doesn’t show or you really just don’t care, you can always use the zirconia called bruxer crown.
Again, it’s about creating a good team around you, trusting the right people, trusting yourself, most of all, to know when to trust and when not to trust.
If you have any questions, feel free to contact me. I have a personal website where I talk a little bit more about my urban farming, my tilapia growing, my trees, a lot of my meditation practice, and a little bit about my philosophy on dentistry, and then, of course, office website and e-mail. I’d be more than happy to answer any questions you have if you feel shy to ask them now or if you come up with questions later.
I’ll leave that up for a couple of minutes, then I’ll put this back.
So, I hope that I brought some good information for you guys, and you can go back and really learn how to really trust your own instincts. With some information, put those things together, like the Chinese, use your heart, use your mind at once.
Thank you very much. So, I’ll open the forum. We have about 10, 12 minutes for questions if anybody would like to. Unfortunately, because of my dentistry, I’ve lost a little bit of my hearing (that zzz). It’s not only bad for the patients, but we lost our hearing a little bit. So, if you could speak up, I’d appreciate it.
Thanks for your information, but whenever there is a dental treatment, there are issues of affordability, especially if you have 4, 5, 6 issues in your teeth. Are there any affordable version as well as better healthy options, especially if somebody wants to go to Mexico and those kinds of things.
Transcribed P2: June 2013: Holistic Dentistry & Biocompatible Protocols (Lecture to Gerson Institute)
Now, the other problem we’re having with amalgams is that an amalgam is very hard, and with time, it starts expanding. When it starts expanding, it starts breaking away from the tooth, and it’s so hard that it starts cracking teeth. I don’t know if you can see here. I don’t have the, but can you see the crack line here? Is that easy to see and one here? Yes, after removing the amalgam, you can sometimes see the crack line, and they’re so common.
I probably do about 30 to 40 crowns per month from people that have had cracks. So, I see a lot more amalgam restorations than most dentists because of what I do, and people want to get them out, but still, in all, it’s incredible. Half the amalgams we take out have cracks on the teeth already if they’ve been in there for any period of time.
So, from the physical point-of-view, the engineering point-of-view, this is a material that’s doomed to fail. Hopefully in five to 10 years, we can be sitting here and this lecture will be stored somewhere because amalgam will no longer be used. That’s my hope, and this is before and after. There’s so many ways now to clean up a mouth to get rid of a lot of those restorations, and we have materials that can actually do the job for us and remove all that toxicity and possibility of cracks. A lot of the teeth crack, and we end up having to think do we need to do a root canal now? God forbid, do we need to extract the tooth? What do we do with the cracked tooth? Sometimes we can repair them. Sometimes we put a crown on them. A lot of time we lose the tooth.
If anybody here has amalgams, when you get home, good thing to really revisit the issue and see if you could get cleared of that, both from a physical point-of-view and systemic point-of-view.
Now, this is one of the biggest questions that I get asked all the time. People call my office, what protocol do you follow in the same person that’s been looking at the internet for two weeks and researching, which is a good thing, and there are quite a number of protocols that people follow. International Academy of Oral Medicine and Toxicology, I’m a member of that. They have their own protocol. Then, Hal Huggins. He’s really considered the father of modern holistic dentistry. He has his own protocol and many variations of the above.
I suggest if you’re going to ask your dentist what protocol he follows, he may give you an answer that you want to hear. I follow Hal Huggins’s protocol. Oh great, I’m coming, or I follow the International Academy of Oral Medicine and Toxicology. Great. So, my suggestion to you is that these protocols are very good guidelines. It’s important, but don’t take your eye off the eight ball. That means that the best of protocols, if it’s not carried out meticulously, is as good as no protocol at all. Again, we’re going to talk about trusting your instincts, trusting who you’re going.
When you find somebody that you can resonate with and you trust, that’s the person that you want to go to versus someone who was recommended to you on the internet or is following such a protocol or another.
For example, one of the most important things in removing amalgams is a rubber dam. A rubber dam, many of you are familiar with, maybe others are not, is just physical barrier. In our office, we set this up, and we actually go in ear and seal it off with a wax so that we have hermetic seal on the area, and you’re not going to be ingesting any of what’s being removed. So, there are a lot of things that dentists must do to remove it safely because you don’t want to remove it like it’s asbestos. You don’t want to remove asbestos unless you have somebody who knows what they’re doing. Otherwise, you’re going to be re-introducing it into the environment, and this is the same thing. You don’t want to re-introduce that into your body.
So, these are some of the basics if you are looking for a dentist that’s going to do this properly. First is you want to prevent the direct intake with a very well-placed rubber dam, meticulously well-placed rubber dam. The other part is preventing gas intake, and that has to do with a good oxygen mask, a good ventilation, a power vacuum. Electric handpiece is one where you can actually lower the rpms and you can actually segment the amalgams so that it’ll come out in pieces rather than to have to grind the whole thing out.
Keep in mind some of these things. This is what you’re really looking for when you’re looking for somebody, or if you want to recommend a dear one in your family who’s looking for the right person to do this for you.
So, in our office, in addition to that, we use homeopathy. We’re very lucky because in our office, we have big windows. We can aerate the whole area often. We do nutritional guidance and quadrant dentistry, which means we take a segment of the mouth. We clean it all at once. We’re not doing one or two teeth at a time.
Well, so now patients are demanding a little bit more healthier alternatives to what we had before, and from the time 30 years ago where people were calling me a quack, pardon the pun here, we’re getting a lot more people following the lead now. So, glad to say that. Glad to report that there’s more and more conscience not just amongst the public, but perhaps because of the public, dentists are beginning to respond.
Let’s shift gears a little bit, and we’ll have a few moments for questions after this, if you’d like. What we’re talking about how we start viewing the human body as sections, as individual sections, and maybe it’s my liver, but nothing functions in a vacuum in the body. Everything is connected, and what have we found about the mouth and physiological connection. Well, a lot of research has shown, particular research has been done on heart disease and how bacterial infections in the mouth actually are affecting the heart.
Now, if you go and do your research, you’re going to find articles that say no link. There’s absolutely no link, and you’re going to find articles that are going to show a definitive link. For me to come and say there’s an absolute link that has been shown scientifically to be the case, not the case. It’s not true. However, they have found that a lot of the bacteria that hide in the gums, and most of you probably know the difference. They’re mostly anaerobic bacteria. Anaerobic bacteria are the kind that doesn’t like aerobics, air. They actually hide in the guys because they’re deadly afraid of oxygen, and that’s actually how they get their colonies to proliferate.
Once you start getting gum disease, and you start getting the space between the gum and the tooth is very important because that’s where the bacteria actually hides itself. Yes, and after we start getting 3 or 4 millimeters of depth in the pockets between the tooth and gum, the bacteria start cheering because, we’re untouched now. They can’t get to me. Right? At 2 or 3 millimeters you can get in with your toothbrush and clean it everyday. Once you get 4, 5 millimeters, it becomes a serious problem because the bacteria are untouched, unharmed, and unexposed to air.
So, this is what we’ve seen the office do, advanced stage. For example, if you see this area right here. If I take a probe, a little instrument, and place it down here. More likely than now, my instrument will go way down here. This is where the bottom of the pocket would be, and we have all this area right here. The toothbrush can probably access that, and all this area down here is no longer accessible and creating a lot of damage.
So, this is what we’re talking about. This is the gum. This would be healthy with very little space here. This is unhealthy when we start having very, very deep pockets here. Now, why am I putting so much emphasis to the pockets in your gums? Because these are the anaerobic organisms that we find inside the gums that we’re also finding in heart disease, same bacteria that we find in a heart that is diseased. Lately, they found the same bacteria in pancreatic cancer. Wow!
Well there’s no studies showing there’s a direct link, but by golly, if I’m finding the same bacteria here that I’m finding here and I’m finding here, well I suspect. I’m concerned. I’m concerned. I would not wait for the definitive research which may take another 20 years for me to know that this is not a good situation, that I don’t want that anaerobic bacteria inside my gums.
So, what do we do? In the past, what we’ve done is basically brushed our teeth, and it’s amazing to me that more dentists do not take the time to teach people how to brush their gums properly. Out of 100 patients that I get, 95 patients have never had any instruction on how to properly brush their gums, not their teeth, their gums.
Part of the traditional hygiene is still very much of great importance. How to
properly brush your gums. I usually instruct my patients to brush their gums just with water and take some time and physically get in there and remove the bacteria from the pockets. Then, they can actually go ahead and put some toothpaste on or whatever they like to use and brush their teeth as a separate activity. I like them to give the gums a lot of attention for the reasons that we’ve already explained, and of course, the dental floss does the job that the toothbrush cannot do.
However, what has happened was that, in my practice, I’ve had people that had come with 5, 6, 7, 8 millimeter pockets. In the past, what did we do with these patients? Well, most dentists would do what we call deep scaling. I’m sure some of you have had it or have heard of people that have had deep scaling. Well, deep scaling is fine and good. It’s a wonderful procedure, but if you’re going to see the dentist once every 6 months and he does the deep scaling for you, what happens between the two appointments? All these bacteria are still growing in there.
The second thing we would tend to do is we would trim those gums back which is called gum surgery. We would cut them back. The gums would get exposed. They’d get very sensitive. It’s probably the lesser of the two evils to have all these bacteria there or to get your gums trimmed back, but it’s not a pleasant thing to have longer roots and sensitivity and all that. I know some of my patients are saying, Doc what else can we do? Can we do something else?
Real Momma Writeup
Realmomma.com did a great writeup for us, introducing the concept of holistic dentistry.
Real Momma: “The latest advancements in dentistry have created a whole new market into holistic and gentle dentistry. I think this is a great alternative to the methods that have been used for many years…”
You can read more about it here:
http://realmomma.com/the-gentle-dental-perspective-on-amalgam-fillings/
Moved from alpha dental

Our Move From Alpha Dental
I am very excited to announce our move to a new, state of the art facility, just 3 miles from our previous location (alpha dental), with easy freeway access and plenty of parking.
All patient records have been securely moved to the new location, where you will receive the same level of care that you have been accustomed to. Please make a note of our new phone number and address for your next appointment:
Call 619-630-7174 for our new location.
About Dr Vinograd (no longer at alpha dental)
Put Dr. Vinograd’s years of experience in every aspect of dentistry to work for you. We provide complete diagnostic services and all treatments in one convenient location. We use the latest technology and materials, including:
- diagnostic lasers and digital x-rays
- injection-free, no-drill fillings for kids and adults
- mercury-free, nonmetallic biocompatible materials for all fillings, crowns, onlays and bridges
- invisible braces
Dr. Vinograd (no longer at alpha dental) has offered state-of-the dentistry for more than two and half decades. Read about his background to learn more about his commitment to high-quality dental care:
Dr. Vinograd (no longer at alpha dental) has been practicing dentistry for more than 25 years and has been committed to biocompatible dentistry for nearly a decade. In addition to his work with patients like you, he is an associate instructor at the USC School of Dentistry and has provided dental services during five mission trips. His D.D.S. is from the University of Southern California. He also has a degree in naturopathic medicine, a degree from Universidad Tecnologica and a BCLAD from San Diego State University. He is fluent in Spanish.
Alpha Dental, Now San Diego Dentist Offerings
Restorative and Cosmetic Procedures
- All-Porcelain Crowns
- Porcelain-over-Metal Crowns
- Porcelain Onlays and Veneers
- Composite Resin Tooth-Colored Fillings
- Porcelain-Fused Metal Bridges
- Porcelain Veneers
- Implant Services
- High-Quality Individual Tooth Replacements
- Oral Surgery
- Crown Lengthening
- Extractions
- Wisdom Tooth Removal
- Emergency Surgery
- Periodontal Services
- Removal of Gingivitis
- Gingival Flap Procedure
- Periodontal Scaling and Root Planing
- Osseous Surgery
- Bone Graft
- Orthodontic Services
- Invisible Braces
- Appliance Creation and Fitting
- TMJ Night Guards
- Sports Mouth Guards
- Whitening Services
- Whitening Trays
- In-Office Whitening
- Preventative Care Services
- Exam and Cleaning
- Digital X-Rays
- Sealants
- Intraoral Digital Photography
- Panorex
Please make a note of the change of address from alpha dental:
San Diego Dentist
(map)
– Daniel Vinograd, DDS.
Transcribed P1: June 2013: Holistic Dentistry & Biocompatible Protocols (Lecture to Gerson Institute)
I think many people over the last several years, as information has become more available, have become aware that there is a large number of people in the field of dentistry who don’t seem to understand that the mouth is part of the body. It’s something completely separate and doesn’t relate to any of your other physiology whatsoever.
We’re very lucky to have with us today someone who does. Dr. Daniel Vinograd is a Holistic Dentist, and he is the dentist to many of the staff at the Gerson Institute as well. He is going to tell you how it might be done in a better world.
Dr. Daniel Vinograd:
Thank you so much. Hello everyone. I’m glad to be here with you all. With this weather, I would expect half of you would be down at the beach so I got to commend you for being here. Who do you trust? We’re going to start out thinking big here to start off the session, but who do you trust?
We have so much information nowadays, sometimes too much information. It used to be that if we had to find something out, I remember, as a young person, I had to actually hire a research team to find out anything I wanted to know or go to library. Now, it’s right here.
So, I get a lot of patients coming in and saying, “Doc, I read this, and this is what is best. This or that.” It seems to me that some people have done some great research, but all of a sudden, they have too much information. They don’t know what to do with it.
I think a lot of that applies to dentistry. What’s good? What’s bad? What materials? Root canals. This. That. So, again, the question is who do you trust? Should you trust me because I’m standing here? Absolutely not, and I’d like to propose to you that if we really start thinking big outside the box, whether you’re religious or not, there’s a concept that I think is important to understand. It’s that if you have a very scientific mind, you have to understand that we are, right now, us, sitting here, each one of you, we’re a result of a billion and a half years of evolution. Wow! Don’t get about thinking big, right?
If you have a religious inclination, there’s incredible godliness in each one of us. So, when I say, “Who do you trust?” There’s really no better answer than yourself. We just need to learn how to listen because we are full of information. Every cell in our body, as a scientist, I think, has a billion and a half years of evolution. What does that mean?
That means learning. Every cell has been learning up to this point. So, when people say, “I have this feeling,” or there’s some intuition, we’ve been learning how to disregard that. The only thing that we should really pay attention to is what our mind dictates, and I think that’s a mistake.
In Chinese medicine, they talk about heart-mind as one entity, and I think they got it right. We tend to disregard and just think up here, make decisions from up here. I think it’s very important for us to really understand to trust our decisions, to trust ourselves, and to trust our instincts. Does that mean that you’re going to make decisions all by yourself without any knowledge? No. Does that mean that you don’t want to rely on experts? No, but you have to use that intuition to know who you trust, what information you trust, who’s trying to sell you something, and who’s really trying to give you information that you can rely on.
Having said that, this is my first point: We really must take responsibility for our own health. We just have to. Why? Because there are so many interests out there that are really looking to get our hard-earned dollars, and they’ll say anything to get into our pockets.
Having said that, there are wonderful people out there. I’ve spent many, many years going down to Guatemala, Peru, and I’ve had interaction with incredible doctors, dentists that give up their time, are incredible people. So, there are lots of people out there that are just incredible people, but corporate America is not necessarily looking out for our interests.
So, from now on or maybe 10 years back, when the corporations basically started taking over and influencing governments to push their agendas, we have to start advocating for ourselves. You cannot trust what people tell you on TV, on the radio, on print. It’s just unreliable now. Is there some truth in some of that information? Yeah, of course there is truth to some of what they’re saying, but we cannot count on that.
So, let’s now talk a little about dentistry, how that relates to everything that we’re actually talking about right now. I remember one of my very, very dearest friends Boris Schwartzman, nice guy from Mexico City. He was studying at UCLA, and he was part of the dental materials program. He kept on telling me, “Daniel, we’re studying this material, and I have to tell you I’m so excited. It’s got so and so compression strength and this bonding capability and this shear strength and this dimensional stability.” He’s talking to me. I say it sounds like I’m talking to an engineer, not a health professional, and, not him, but the whole department is looking at this.
I say has anybody really thought about the physiological effects of these materials? After all, we’re not going to be constructing robots. We’re putting them on people’s mouths. So, I kept on asking, what about the biocompatibility of these materials? Is anybody studying that? You know, I mean, I wasn’t born yesterday, so it was about 30, 35 years ago that we had this conversation.
So, this is the result of that kind of thinking. Where they thinking evil thoughts about poisoning people? No, I don’t think so. It was just the disregard that the thinking was one of looking at materials to see what is going to be strong enough to withstand masticational forces, which is really a big part of dentistry, too. You have to have that as well. So, that resulted in dental amalgams, formaldehyde being placed in children’s mouths. It’s just a great deal of evidence showing how a lot of these materials are so toxic. You wonder, how is it that we even thought of putting them in people’s mouths to start off with.
We’re going to show a little bit of evidential studies that show how the body, the mouth and the body are connected. Part of the Industrial Revolution and the specialization created doctors who became more and more specialized, and all of a sudden, this guy was a specialist in lungs. This guy was a specialist in the right toe, and by the end of the day, we’re looking at little microcosms of things that we really stopped separating everything. We started separating the fact that every part is connected? Everybody knows that song, right? There should bone’s connected to the… Right? It’s all connected.
So, again, traditional root canals were a result of that as well. People just looking for some kind of very practical way to solve a problem. Did they solve some problems? Absolutely. Did they bring other problems? About absolutely.
Let’s talk a little bit about mercury amalgams, and this is quite interesting. In 1833 is when they first came. Amalgams were brought to this country by a couple of Frenchmen, and people started going crazy for amalgams because all of a sudden, you had something hard that you can place and people can go back and chew. So, that was yay! Let’s hear it for amalgams, but these were our heroes. The Society of Dental Surgeons, ASDS, those are the first guys that dressed up in Batman and Superman uniforms, they had this awareness back, in 1844, in saying mercury is one of the most toxic substances known to man. If you wanted to be part of them, and they were the most prestigious institution, if you wanted to be part of them, you had to sign something saying that you would not use amalgam.
So, wow. Back then, somebody had some awareness, but soon after that, by 1856, this group disbanded. The present American Dental Association took over. Is the American Dental Association the enemy? No, but again, they have a certain focus. They have a certain history.
There was a big component of the new American Dental Association that was called, the American Amalgamist Association that was really a subgroup of this that were really pro-amalgam, and this really where the foundation of the use of amalgam. However, we know that mercury is one of the most toxic elements known to humans. How are we living with that? Some people are saying the amalgam gets mixed, the mercury gets mixed with a lot of silver and cadmium, and it gets fixated. Who knows? I don’t know that, and whether it’s true or not true do I want to have that in my mouth?
There’s good studies that show there is leakage of mercury. So, I’m convinced. Even if people are not convinced, they say, amalgam’s really stable. It doesn’t hurt anything, but why would I want to take a chance of putting something that 50% mercury in my mouth?
Now, this is not me. This is not some holistic dentist telling you this. This is the department of health and human services, the United States government is telling you that mercury is the number three toxic element that they have found. So, in 1970s, I began asking my colleagues to stop using amalgams. Do agree that mercury is toxic? Yes, I agree that mercury’s toxic. Well, whether we find out or don’t find out, why would you want to start using this? Why would you want to use this at all? Mostly the answer that I got.
Why isn’t your dentist telling you what’s on the label? These are the labels from amalgams. You can read for yourself what the manufacturers are telling you, or me, as a dentist, about amalgam, and I know, in this country, amalgam is still widely used.
So, we can’t change the world all at once, but it’s people like you that have awareness, that care, that are here instead of sitting out on the beach, that this message is important for.
This is what I see in my practice every day. These are amalgams. These are restorations. There are a couple of problems with the restorations. One, from a biocompatible point-of-view, we’ve already discussed the content of one of the most toxic materials there are, and as time goes by, they get oxidized. They break up. They start leaking. So, this is very common place in every dentist’s practice. This is what we’re seeing after amalgam’s been in the mouth, and you’d be surprised. I’d ask a patient, how long as this been in your mouth? Some of them would say, “Since I was a little kid.” Other people would tell me two or three years, and amalgams start looking like this.
Toward the First Revolution in Mind Sciences P6
Final point here is I suggest that toward a first revolution in the mind sciences; I would suggest that we haven’t had one because there’s been too much dogma suppressing the empirical study of mental phenomena themselves, as opposed to the physical correlates. But now there’s a possibility, as we have access to Buddhism and Hinduism, the Sufi tradition, psychology, neuroscience – we no longer are isolated. Here at Google, you know this maybe better than anybody else. You are on the globe. Your physical plant happens to be in Mountain View, but it could be in the Amazon. Right? We are now living in a globe where we can integrate like never before.
Integrate these rigorous first-person and third-person methodologies, from the contemplative, the psychological, the neuroscientist, in collaboration between cognitive scientists – the whole broad range – and contemplatives who have exceptional mental skills and insights resulting from rigorous sustained mental training in observing and experimental with states of consciousness. So there would be a challenge, to break down the barriers, to throw out dogma and uncorroborated assumptions, and open up a new renaissance of empiricism in the scientific study of the mind that would be profoundly contemplative and experiential and yet rigorously scientific.
That could revolutionize the contemplative traditions; it could revolutionize science; and it could bring this unfortunate rift between religion and science, creationism and the school district that makes most of us gag, and so forth, breaking down those barriers, and see about integrating East and West, ancient and modern, and cast a fresh light on the nature of the mind and on human identity. It’s a possibility. That’s my hope.
If anybody has questions or observations or debates, anything is welcome. Yes?
SPEAKER: [Inaudible 00:55:19] ask a similar question [inaudible 00:55:22] came back to [inaudible 00:55:26] instead of looking so much at Buddhism, looked at the split within the Greek thought as one of the original ways to be able to look at resolving this. Then there’s also, of course, Ken Wilber, who [inaudible 00:55:39] a particular place, look at all the traditions. Can you just comment on why Buddhism [inaudible 00:55:47] just one way, or…
WALLACE: It’s just one way. I was using that in a short presentation. I was saying, “here’s a good sampling.” This was not promoting Buddhism versus Hinduism or the Muslim tradition or the Daoist tradition. Not at all. I was saying, this is a good example, from the very rich, well-developed, intellectually very sophisticated contemplative tradition.
But the Santa Barbara Institute, which I founded, is not a Buddhist institution. It is an inter-contemplative tradition, drawing from the wealth of East and West contemplative traditions from all over the world, interfacing these with the best of science. So it’s not plugging any one tradition, and it’s certainly not trying to validate Buddhism or any particular school. Very much to the contrary. These great contemplative traditions have been after universal truths, and not just trying to corroborate Buddhist ideas, and I’m not interested in that at all.
So I think, going back to Greek thought, back to Plato, back to Pythagoras, themselves, to the notion of noetos, which is a type of mental perception by means of which we can directly observe non-sensual mental phenomena – that’s a Greek notion, but we’ve forgotten it. So I don’t want to leave anybody out. That is, indigenous people, East and West, bring it all together, because the stakes are high now. We’re dealing with something that is central to everybody’s existence, and that is consciousness.
So let’s throw out dogma of all sorts, sectarianism, biases of all sorts, and not leave anybody out. Not leave out the contemplatives, not leave out the neuroscientists, for heaven’s sakes. Not leave out anybody. And really start fusing and taking advantage of the technology, including transportation, that we have now, so that we can really draw from this wealth of wisdom and insights and multiple methodologies. This epistemic pluralism I think is absolutely the key.
Two more questions. Here’s one.
SPEAKER: If you want to approach consciousness in a scientific way, which I assume you –
WALLACE: Absolutely.
SPEAKER: – are for, you need some idea of what it means to prove or disprove something. How do you do that in the absence of physical observation?
WALLACE: Very good. The question is, if this is going to be scientific – and of course, science gained its laurels by studying objective things, that you can look at it from a third-person perspective; quantifiable, but measurable out there, right? So if one lab does it, another one can corroborate it and it’s pretty clear. Mental phenomena are subjective. There we are. They’re, as John Searle says, “irreducibly, ontologically first-person.”
But I think a good analogy for this – the question deserves not a two-minute answer; it deserves conferences and really detailed investigations, so we don’t come up with cheap answers. Cheap answers are easy. But if we take as an example mathematics. Mathematics is not scribbling things on a board. That’s the outer display of it, but anybody who doesn’t know mathematics can memorize the equations and write with the best of them, with no understanding at all.
When I studied higher mathematics in my training in physics, it’s subjective. It’s working through a proof, it’s thinking, and you may do something out here on the board, you may not, but the real juice of mathematics is something that’s taking place internally. How can mathematicians ever speak with each other? How can they know who is great? Well, they get a similar training. They go through an undergraduate, they go through the graduate, they go through post-doc.
After awhile, they know who gets the Fields Medal. It’s not just that he wrote things on the board; it’s through dialogue. You say, “We speak a similar language here. Everybody else can’t understand what we’re talking about, but you and I have gone through eight years of training and mathematics, and we know the elegant proofs. We know shoddy mathematics. We know the sharp stuff.” So even though it’s largely internal, they develop a language, a common training, so they can communicate amongst themselves in ways that outsiders cannot fathom.
Let’s imagine – this is hypothetical in a way that is also historical in another – and that is, I spent a lot of time with Tibetans, living in Tibetan culture. We have contemplatives there who will go for 10,000, 20,000 hours of training, with a common basis of ideas and training, contemplative technology, and so forth, and they develop a refined professional language. That they can speak amongst themselves, and they know what they’re talking about, because like the mathematicians, they share training and developing, they share a vocabulary.
And we know this is true: in the Tibetan tradition, all the great contemplatives, the great scholars, they know who the cream are. It was Dilgo Khyentse Rinpoche, it was Ling Rinpoche, it was Kalu Rinpoche. These people, the peers know. To an outsider, it looked like a really sweet monk, really nice guy. Good charisma. But the professionals know it’s more than that. This guy really has the skivvy. This man really knows what’s going on. I would not ask you to accept that because I’m saying it, but I am saying this issue has been grappled with.
If we take a more prosaic example, wine connoisseurs. That is, when I drank, I got my pallet ruined when I was 18 because I got drunk on Red Mountain wine, whiskey, and beer in the same time, and that totaled my tongue for life. I can’t tell any good vintage from another. But I’ve hung out with people who have had that training. It’s three years formal training, and then years of getting experience. So two wine connoisseurs will come together and say, “Was it a 1948 or ’49, and what part of France was this raised in?”
The taste of wine is very subjective. You can’t pick up the taste of wine with some external technology that will tell you this is a $500 bottle as opposed to a $5 bottle. No technology will tell you that. But they train, and then they use things like bouquet and so forth, words I don’t even know what they’re talking about; but they have a specialized vocabulary, and they know who the brilliant wine connoisseurs are and who are just mediocre. It’s a specialized vocabulary that they know what they’re talking about, and outsiders like me, I don’t have a clue.
Wine testing, that’s very empirical; the mathematical is very internal. If we try to draw inspiration from those only by analogy, then perhaps we can get some idea. But again, the danger – there’s all kinds of potholes here, a minefield, and that is they’re all being brainwashed in the same way. That was how introspection fell to its knees and died, is that different labs were simply corroborating their own assumptions, and the trainees, the observers, their observations were so laden with the theories and assumptions of their mentors that they weren’t getting this inter-lab corroboration. So it fell apart.
But they gave up too soon, and they didn’t go through a 10,000 or 20,000 hours’ training. Not Wilhelm Wundt, not Titchener at Cornell, not James at Harvard. This requires training. If it’s going to be professional, don’t give them five hours of training or a week of training; how about three years of training, ten years of training? Train in the mind ten hours a day.
previous_post()


 Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here:
Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here: 
