Dental Implants vs Dentures (Podcast)
Podcast: Play in new window | Download
Hello, this is Dr. Daniel Vinograd, biological dentist in San Diego, California. Today, I’d like to talk a little bit about dentures and denture alternatives. If you really think about what dentures are, couple of these little plastics, a little bit like castanets, they’re going against each other trying to mash food together. The concept is a little bit foreign, and it’s a little bit unusual. However, it’s certainly better than not having anything at all.
The truth though is that a lot of people will resign themselves to wearing dentures. At least they have some teeth to show for it, but the mastication is quite reduced, and the quality of life is also not great. There are a lot of issues with sore spots, with bone being reabsorbed, creating dentures to not fit as they should, needing realignments and so forth. Eventually, with time, the bone will reabsorb to a point where the dentures are hard to really keep in place.
A little history. Dentures go as far back as 700 B.C. were being made with animal and human teeth, and they were put together in some contraption. People would use them to try and show that they had teeth and try to do some chewing. That lasted for quite a while. Even up to the 15th century, you’d still have those dentures that were made out of human teeth and animal teeth. I can’t even imagine how uncomfortable and unsightly they were. Of course, we don’t believe that they had any kind of extended use. Around the late 1700s, modern dentures came to be with the advent of modern materials, and this is basically what we are today.
Now, a lot of people feel that once they’re in dentures, this is really their destiny. A lot of them have gone through a lot of dental work, and they slowly but surely have lost their teeth. A lot of our grandparents used to wear them so we became comfortable with the thought that dentures were a normal part of getting old.
The truth though today is that there’s so many alternatives to dentures that can really improve the quality of a person’s life so dramatically, and all of them are really based on the use of implants. Implants, even 20, 30 years ago, were not really considered to be mainstream dentistry. I remember placing one of the first implants, and a lot of my colleagues did not look favorably upon this kind of a procedure. Today, dental implants have progressed to the point that if properly done and properly integrated, the success rate of implants is better than 95%, and implants can actually be used to replace dentures or in conjunction with dentures. So, here’s they work.
There’s actually two ways that you can use implants to improve the quality of life of a denture wearer. First, is you can actually use implants and place an overdenture on them. What you would do is basically, you would use the denture with a couple of female pieces and attach it to a male piece that would come out of the implant. So, in essence, the dentures are actually buttoned into the area in your mouth where the implants were placed, holding it firmly.
Dental Implants / Fixed Restorations
The second way that you can actually use implants is by getting rid of dentures altogether, and you can actually place as many implants as there is bone available, and you can actually place individual teeth to replace the teeth that were lost.
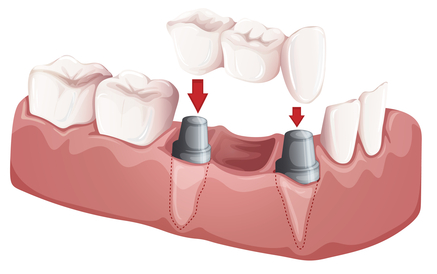
Finally, there is another way of doing it which is placing anywhere from four to six implants and then laying an underpiece to the denture, usually made out of fiber, and then, you can actually permanently cement teeth into that fiber underpiece. This would actually be a fixed, not a removable restoration, which acts pretty much like bridges would on regular teeth.
One of the biggest considerations here is the amount of bone that is left on the patient. So, obviously, earlier in the stage of denture wearing, you would probably, in most cases, have more bone than you would have alter in life. So, this procedure would be well-advised for people who are just wearing dentures or haven’t been wearing for a long time. A lot of patients who have been wearing them for a long time will have conserved enough bone to be able to place some implants, either an overdenture or a fixed prosthesis. So, that is basically the limiting factor.
There are ways to graft bone, and most of the time, it would have to be a bone graft from your own body, usually your hip. You can actually place additional bone there to be able to sustain some implants.
Once you have those implants in place, the difference is just staggering, and I know patients all the time talk about the fact that they could not have imagined how their lives have improved by actually having something fixed and solid again to chew with.
So, I hope this was helpful, and until next time.
Toothaches (Podcast)
Podcast: Play in new window | Download
Hello, this is Dr. Daniel Vinograd in San Diego, California, biological dentist, and I just wanted to touch base on pain, particularly tooth and gum pain. Basically, I wanted to give the listener an idea of what are some of the expectations and a little bit of what dentists like myself would ask in order to assess the type of pain and what it could mean. So, obviously, my disclaimer is that any of this is just to give you ideas so that you know when it is more likely that you need help or not, but, obviously, ultimately you have to have a proper diagnosis by your dentist.
So, pain is, it sounds like pain is pain, but it really, it could be quite nuanced. First of all, we have to try to decide which kind of pain or what flavor of pain, if you will, your experiencing. We could kind of find out what it is that we may be looking for. If you are having pain that is provoked, in other words, touching of tooth the tooth or gum, cold or heat, makes it hurt, but as soon as this provoking agent disappears, the pain goes away, are usually less worrisome that if you would have unprovoked pain which is pain that would come all of a sudden. As a matter of fact, one of the indications for immediate treatment is when you have unprovoked pain of great intensity, the kind that would wake you up at night. That, I would actually seek immediate help for.
Aside from that, we could talk a little bit about the difference between hot and cold. Usually, when you’re having discomfort with cold, you have some sensitivity, and it’s usually not incredibly worrisome. Hot would be a little bit more concerned about. As I said, the most important thing would be if it’s provoked or unprovoked.
Another differentiation that you can make is whether you are having acute sharp pain or if it’s throbbing pain. Sometimes, I’ll describe the differences with pain like you would be hearing a flute or a drum. The throbbing pain is more like a stomachache. The acute pain is more like a headache, and usually the acute headache type-pain, it’s not a headache, it’s in your mouth, it would be more descriptive of toothache or bone ache while throbbing pain is usually an indicator for gum pain. Obviously, in addition to pain, you would look for other symptoms. If you have bleeding or pus coming out, obviously those would be other symptoms, but you would like at them in conjunction to the pain.
Anyway, anytime that you have any concerns, you should call your health professional and just thought I’d give you a little bit of what some of the indicators are for pain. Typically, when patients come to the office and they’re not sure what tooth or what is paining them, I’d likely tap on the teeth to try to really ascertain which tooth it is, and obviously if there is one particular tooth that responds to the tapping, we call it percussion, that will give you a better idea of what tooth you are looking at.
Again, sometimes when it’s diffused, pain can be projecting itself into other areas. We call this referred pain. So, sometimes it is a little bit tricky where the pain will start at some area, but you will feel it radiating into some other area. That’s because we obviously have a network of nerves throughout the mouth that are connected.
So, I hope that this was helpful to you, and I hope that you have a great day.
Feel free to call or e-mail with any questions: (619) 630-7174 / [email protected]
Dental Implants: The Biological Perspective (podcast)
Podcast: Play in new window | Download
Good morning. This is Dr. Daniel Vinograd, a biological dentist in San Diego, California, and today, I’d like to speak a little bit about dental implants. So, it’s interesting how much implants have actually progressed over the last couple of decades. I remember, maybe over 20 years ago when I first started placing dental implants, I was considered a little bit on the fringe.
Dentists who placed implants were not looked upon very favorably. In fact, there was a lot of pressure on people who started placing dental implants, and it was considered, pretty much, outside of the realm of dentistry or at least prudent dentistry as some people saw it. There was some truth to that because they’re quite invasive. There were large blades that were placed on the mandibles just to restore one tooth.
So, fast forward 25 years, and now, we’re really looking at dental implants as the fastest growing area in dentistry in one that has possibly got a 50% success rate to over 99% success rate if done properly. So, this is probably an important consideration for most patients that are either going to lose a tooth or have lost a tooth that is important for their function.
Now, in the biological point-of-view, a lot of people ask me what I think about dental implants, what I think about root canals, etc., and my biggest concern is actually from a biological point-of-view is obviously bacterial infection. When you have a root canal that is the focus of bacterial infection or a tooth that is quite involved periodontally where the gums are inflamed and infected, that, in itself, to me, is a much, much greater challenge to the body than anything else.
So, having said that, when do we decide to place an implant versus, let’s say, a bridge or a root canal? A lot of those considerations have to do with your general health. Also, important to look at, for example, if you have two adjacent teeth lost or to be lost that have large restorations, I would probably consider placing a bridge there because, really, there is not going to be a great loss. As a matter of fact, sometimes, it’s an improvement on the adjacent teeth. However, when you have a couple of virgin teeth on each side, then you really, definitely need to look into an implant.
Now, what are the considerations for a dental implant? What are the requirements? Mostly, it’s just about having a healthy bone which 95% of the population has, but also, you need to have enough bone for an implant to be placed. There are a number of different dental implants in the market, and when the modern generation of implants came out, people were placing implants that were quite, quite big, 18-, 20-millimeter long implants which is really quite a huge implant and quite invasive.
In the last decade or so, dental implants have gotten smaller. As a matter of fact, there are a lot of research papers that have come out showing that smaller implants integrate better and have equal longevity to longer implants. So, really, the movement has been towards shorter, better designed implants.
Today, a lot of dental implants are in the 10-15 millimeter range, which is still large and invasive, not compared to where they used to be, but there are other options today which I’d like to talk about. That’s mini-short implants. Now, there’s a difference between the mini implants that are placed for dentures, which are very thin, and implants such as Bicon which is the ones that I use. They’re actually much shorter but very well-designed, and they have a lot of surface that a bone can integrate to.
So, usually, my dental implants are about 6 millimeters long which actually makes a huge difference in my ability to place them without being so invasive, without needing so much bone, and that often translate to not only a less invasive procedure but a shorter recuperation time and often less costly. That is because often when we don’t have enough bone, we have to actually look at either grafting bone into the area, repositioning nerves, or actually lifting sinuses to create space for the implants. Those are all invasive procedures, and they are also a bit costly and, obviously, problematic as far as possible complications and bringing new variables into the equation. So, the ability to place a 6 millimeter implant allows us to have tremendous versatility, lowering costs and allowing us to place in some areas where a regular implant would not be placed.
A lot of people at the beginning were actually doubting how sturdy or how much these dental implants could actually last, and all research has shown that they are equally effective, efficient, and actually a little bit more successful than some of the longer implants.
One of the important aspects on implants from a biocompatible point-of-view is the material that the dental implant is made from. Most implants, I would say, a great majority of them are made of titanium, which is probably the most biocompatible metal there is. In Europe, they have been using zirconia implants, and I know a lot of people ask for zirconia implants. There’s not really a problem with the zirconia itself. Actually, it’s very biocompatible.
The problem is the zirconia implants are one piece. They’re very long, very invasive, and by being only one piece while most of the titanium implants are two pieces, you actually have to place this implant in a perfect position to be able to place a crown on them. That actually translate often into a need for the dentist to re-prepare the top part of the implant where the crown is going to go and create some microfractures. So, there have been issues with fractures, and there are issues with them being very invasive and really difficult to place, making the outcome less certain.
If you would have tremendous amount of bone and easy line of insertion for the implant, they could work quite well, but in most cases, it is a challenge. So, for that reason, I have shied away from them. I understand in Europe they are working on a two piece zirconia implant, and when that takes place, I will revisit that.
 In the meantime, the fact that the Bicon implants are so short and so small, they seem to be so uninvasive that, at this point, I favor those, and that’s definitely what I would place on myself or a family member. In addition to that, we need to think about the possibility of getting those implants with biocompatible materials that coat them, making them more biocompatible.
In the meantime, the fact that the Bicon implants are so short and so small, they seem to be so uninvasive that, at this point, I favor those, and that’s definitely what I would place on myself or a family member. In addition to that, we need to think about the possibility of getting those implants with biocompatible materials that coat them, making them more biocompatible.
Ultimately, there’s a lot of research. You can go on the internet and seek a lot of information out. In my practice, I just really am very observant, and most patients talk to me a lot. When I see that a procedure is actually being well-received by most people’s bodies, most people’s jaws, that in itself is very reassuring, and what I see in the dental implants I placed is the body really loves them. They get integrated quite nicely, particularly the design of these Bicon implants. There are very, very few problems. Leakage used to be a problem with a lot of them, and the design of these as well as a few others that have improved on their design are really now at a point that if they are well placed, they have over 99% chance of success.
So, I hope that has been helpful. I have really expanded the place of dental implants in my practice because I feel it’s a very clean, a very successful procedure that has actually been well-received by patients, both in its function and its biocompatibility.
All the best and I hope you all have a great day.
11/13 Lecture: Holistic Dental Health (Transcribed) P5
Removable bridge. For some people, successful. They have a lot of tolerance. They put that in, out. They’re comfortable. They feel good. From a biocompatible point-of-view, one of the best answers. From a lifestyle point-of-view, one of the worst answers. It’s very, very difficult to have a good quality of life when you have this thing in and out of your mouth.
Fixed bridge. Now, we can actually do very nice fixed bridges without any metal. Advantage, you replace it. It’s very biocompatible, but disadvantage is that you have to grind the two adjacent teeth. If you have two adjacent teeth that are broken down, have fillings, then it’s a no-brainer. If you have two very good teeth, nice quality teeth on the two sides of that tooth, I would really think twice before I go ahead and grind those teeth down.
Then, a Maryland Bridge, which is a much more conservative three-unit bridge where you don’t grind the adjacent teeth quite as much is a very nice compromise, but it is a compromise because those bridges tend to get dislodged.
So, again, the magic pill isn’t here, and I’m not here to give you a magic pill. I’m just giving you facts so that you really can make good decisions again. This is a design of a Maryland Bridge.
Now, let’s talk about root canals, biocompatible root canals. I really stopped doing root canals for about 20 years because I just saw what was a root canal and what a really poor job a root canal was doing in really sealing off the canals and preventing biological invasion.
Today, there’s a material called BC Sealer, which is a calcium-based material, which is a very biocompatible, osteogenic, which means it actually helps bone being laid out that is being used in a lot of parts of the body to actually promote bone growth. It’s also hydrophilic. This is the key. Hydrophilic means that they like moisture, and what does a material do when it likes moisture? With slight moisture, it tends to absorb a little of moisture, and when you absorb the moisture, it expands. So, it expands, and it creates a much better seal.
The other advantage of BC Sealer is that it has a pH of 12.4. No living organism survives at 12.4 pH for very long, and this material actually takes 48 hours to set. So, it’s actually actively disinfecting the canal for 48 hours. So, now, I’m doing again biocompatible root canals, and, so far, in seven years, I’ve had zero failures so far. I mean, I may have had some that I don’t know about, but they’ve been quite.
Now, having said that, if I have a person that has a lot of challenges like cancer, some systemic challenges that are very serious, would I consider extracting a tooth and not doing a root canal? Of course. I may want to do that for a patient that is immune-compromised. If I have a very healthy patient that is not immune compromised, and this is a particularly important tooth where having that tooth out is going to create a lot of challenges in your lifestyle and your quality of life, I would not hesitate to do a biocompatible root canal.
So, again, you’re going to hear a lot of pros and cons, and you still may disagree strongly with me, but at least now you have some idea of what’s available and what the problems are with root canals. Okay. Again, you know, it’s your responsibility to take your health into your own hands, and I know I don’t have to tell you this. You guys are here. This is the wrong group to be preaching to absolutely.
You guys are the exception. You are the cream of the crop. You are aware. So, I don’t have to remind you too much about the fact that in the last decade or so, corporations have basically taken over the decision-making process in this country and in the world where I don’t know if anybody saw this documentary called “Corporation”. Corporations, really their only requirement is to make profits for their shareholders. There’s really nothing that says there that they have to be moral, that they have a responsibility to the greater good. Nothing.
So, legally, they actually have the responsibility to make money before they have a responsibility to create a good product or a health product. What does that mean? That we have to really make decisions now for ourselves. So, there are great number of people out there that are going to help you do this.
There are a lot of very committed people. I often go to missions, dental and medical missions in Guatemala and Central America. I meet some amazing doctors, amazing dentists with their heart in the right place. So, people are out there to support you, people that are doing the right things for the right reasons. Your job is to find them, and to make them part of your network.
Again, this is my personal website. You can get a lot of information there. Personal website about not just about dentistry but how I grow my own fish and my own vegetables and how I make my own toothpaste, a little bit of a more personal website. Actually, my son built that website for me, and I told him that’s a great memorial. I can die now and leave something behind.
Then, there’s our office website and personal e-mail if you guys have some questions. Of course, I’d be more than happy to communicate with Gerson with any questions that you might have. You can ask them through the Gerson Institute.
Do you have time for just a few?
Absolutely. Please. Yeah, speak up because the drill over the ears has actually taken a toll. So, you have a root canal with a tooth broken, and it’s kind of deep. You want to get rid of the tooth and put in a fixed bridge. How long would you wait for that to heal before you would do it?
Well, in our office, what we do is we extract the tooth, we prepare the adjacent teeth for a bridge, and we put a temporary. Then, we wait from six to eight weeks with the temporary bridge in place for that area to heal. The reason you want to put a bridge there is because as soon as you extract the tooth, the teeth tend to collapse into this space.
So, you actually want to stabilize that area first, but you don’t want to make that bridge prematurely.
Otherwise, you still will be healing underneath the bridge, and you have a gap in between.
How hard is it to pull the rest of the tooth out?
It just depends how much experience you have.
Yeah. Thanks, man.
I’m sorry. Could you raise your hand? There was another one here some place.
Gold inlay. What are the complications of that?
Gold, as a material, has been used over many, many years. It’s a good material. It’s more biocompatible than many other things, but you have to realize that gold is not pure gold. If you use pure gold, it would be wonderful from a biocompatible point-of-view, but pure gold is too soft. So, the gold has to be mixed with copper, with tin, with a few other things. So, it’s still a good option. I would say that today bruxor inlay would be more biocompatible, a better solution altogether. Does it mix well with the bruxor? Yes because it’s basically not a true metal. It’s just a porcelain piece. So, yeah, it would.
Can you just repeat what he said? He was asking if.
He was asking if it would mix with gold or other metals in the mouth.
I have a dentist like what you mentioned at the beginning. He’s into business, big money maker, but I’m looking for a dentist that is more economical so that this can get done. Does your website mention resources in different cities in this country?
It doesn’t, and I really don’t know enough good dentists everywhere to recommend them.I know a few. So, you can always e-mail me, and I’ll see if I can help you out with that, but most importantly, ask questions, see how people are doing, look into people’s hearts why they’re doing what they’re doing. Then, take responsibility. Take this information and make sure they’re applying a lot of these basic concepts in the way they’re taking care of you.
Do you recommend that people go to the IONT as a starting point?
It’s not a bad place. Most of these places where they list dentists, all you need is to pay your dues and become part of their group. So, unless you’ve done something really wrong, they kick you out. So, it’s not a bad place. It’ll weed a lot of dentists out, at least the dentists that have this kind of vision or are trying to work within the parameters, but that does not guarantee that you’re going to get somebody that’s truly biocompatible.
You could start with a list from that in your area, and then go from there.
Absolutely. You can go interview the dentist, but I would still interview the dentist.
Regarding the BCC Sealer, or is it just BC?
BC Sealer.
Is it BCC Sealer or just BC Sealer?
BC. BC for biocompatible. It’s actually not biocompatible. It’s bioceramic, but you can remember it by BC.
I have a question about that. That’s for root canal, is that something that since it’s new, it’s not as harmful as others. Is that something they can use on children’s sealants because they’re putting sealants on young kids to keep it from getting cavities on their molars?
No, no. This is strictly for root canal. This is really not strong enough to withstand the masticational forces. So, you use it inside the root canal, and it’s very good at sealing the canal, but it’s not something that you can use in children’s sealants.
Is there one that’s better that I can ask for?
Yup. See, when it comes to sealants, when they’re not placed properly sometimes sealants are worse than no sealants at all. I’ve seen often sealants coming undone and a lot of decay getting in between the sealant and the tooth.
So, you have to make sure that they’re placed properly, number one, and number two, all sealants are basically composite resins. So, you have to go back to what we talked about which composite resin you want to put in there, the one that has the BPAs or the one that was small amounts of fluoride.
She promised us this would be really fast.
Actually, do you know any other professional who can answer? I just wanted to know with the ozone machine, can it be used for other purposes other than just the importance of?
Yes, an ozone machine can be used for multiple purposes. People use them to disinfect rooms, their cars, or whatever. I don’t recommend that you use it for any purposes in which the ozone goes into the air because it tends to create a lot of irritation on your respiratory tract, but once you place it in the water, you could actually use it for multiple things. Any place that you can use that to actually kill anaerobic bacteria, you can use it for, You could actually irrigate a wound with that.
If you already have a root canal with a toxic sealant, can you have it redone using the biocompatible sealant?
Excellent question. We end up in our office doing a lot of retreatments, but really the key is often when you have had a root canal, often dentists will place a metal post in the canal to rebuild the tooth, and then put a crown on it. We don’t use metal posts, and a lot of dentists have given up metal posts because they found the metal posts actually end up cracking the roots and creating a bigger problem.
So, if you do have a metal post in a root, usually that tooth is not retreatable. If you don’t have a metal post, depending on what materials they used, it can be retreated. I find other people come to get retreated about 60%, 65% of those teeth can be retreated, and the other 35% are not. We’d be happy if you want to send an x-ray of your tooth so I can give you some feedback on that.
Well, we can’t keep him here any longer, and he talked a lot about options. I think probably you’re all thinking two options: One, you’re going to stick him in your pocket and take him home with you, and the second one is all of you from out of town are going to move to San Diego so Dr. Vinograd can be your dentist.
Thank you so much, Dr. Vinograd. This was just terrific.
Thank you. I appreciate your time being here, and I commend you all. Thank you to the Gerson Institute. They’re a magnificent institution.
And he is Dr. Smith’s dentist. So, you know, she is incredibly picky so.
Thank you very much.
You’re not allowed to leave without turning in your evaluation. So, we are at the end, and I just want to tell you it’s been so wonderful spending the weekend with you guys. I wanted to leave you with one thought also, and I’m not making this up when I tell you this. This is absolutely true.
Right now, mental health professionals are actually treating people for a condition that they have created called orthorexia. Orthorexia, by definition, someone with orthorexia, is an individual with an unhealthy obsession with clean, organic, and healthy food. They are actually prescribing psychotropic drugs to treat this condition.
Again, I am not making this up. After you leave here this weekend, you may have contracted this disease, this problem with your mental health, but I just want to let you know that I would be thrilled to sit in the loony bin with every one of you, and we will all toast each other with a healthy glass of carrot juice.
Again, thank you very much for giving us these few days out of your life.
Be well. Safe home and stay bold.
11/13 Lecture: Holistic Dental Health (Transcribed) P4
Then, of course, you want to go to your dentist to make sure that he’s probing. If your dentist is not probing your teeth when you go to see him, I would probably ask him to do that or go to somebody else that will do that for you because this is a critical part of maintaining your health. The other thing is that people don’t realize but crowding on your teeth actually creates a lot of gum pocketing and gum disease. So, that’s something that you might want to consider.
Braces were not for adults for a long time, but nowadays, invisibly braces are great, and about 80% of my braces now go on adults. So, that’s something not just for aesthetics, but if you have a lot of crowding, that’s really promoting gum disease. So, something for you to think about.
A lot of times my patients ask me if the trays that you use for Invisalign or Clear Correct, which is a competitor, if they are BPA-free, and they are. Okay, questions about this segment? Yes?
No, you don’t have to. You can keep yourself form getting diseased by using the water pick and the ozone.
Most of the bacteria that cause problems in the mouth, decay, periodontal disease, and endodontic problems, most of those bacteria are anaerobes. There’s studies where they should the combination of aerobic and anaerobic bacteria in our mouths. When there’s disease in the mouth, the anaerobic bacteria take over. So, by actually maintaining the population of anaerobic bacteria in the mouth down, you are keeping disease down. So, yeah, it’s not only when you’re diseased. Prevention is obviously the best answer.
I understand the crowding of the teeth that you were talking about a few minutes ago. What about when you have gaps on your teeth? Does that open up for?
Gaps in your teeth are not problematic unless you have a very small gap in between the teeth where you’re getting food trapped. If you have large gaps, some people genetically just have large gaps in between their teeth, that’s usually not a problem at all for gum disease, and you’ll know when the dentist probes you. If you have a pocket there, it’s a problem. If you don’t, it isn’t basically.
It’s only when there’s very narrow spaces between the teeth where food is getting trapped and actually impacting the gums that it becomes a problem. Yes?
Oil pulling is wonderful. I think it’s a great therapy, and it’s been used for a long time. I’m very pro it. I, actually, because of the great results I’ve had with ozone, have actually, it’s the treatment of choice in my eyes.
The question was, “How do you feel about oil pulling?” Does everybody know what oil pulling is? It’s where you put a table spoon of organic oil, oftentimes it’s organic olive oil or organic coconut oil, and you keep it in your mouth. You swish it vigorously in your mouth for about 10 to 15 minutes. Some people do it for less, but really get the effect. It has to be, I believe, for at least 10 minutes. That’s pulling a lot of toxins out. Then, you spit it out and make sure you get every last drop of it out of your mouth because you don’t want to swallow any of that back down. That’s oil pulling.
So, oil pulling is actually quite good, especially if you have metals in your mouth, it is actually beneficial, but really, a lot of the toxins in the mouth are produced by bacteria. So, if you’re really taking care of the bacteria, you’re really taking care of most of the problem.
Now, having said that, I use most of my own home made paste in our office and I encourage my own patients to make their own toothpaste at home. This toothpaste has a base of virgin coconut oil. We use that, and then we use that and a few other ingredients, but the base of coconut oil gives you exactly the same kind of effect, especially if you brush or a prolong period of time. It would be like a short mini-oil pulling session.
There’s a question from the live stream, Dr. Vinograd. It says, “Where do you buy the ozonators?” Now, I assume that means if you already have a water pick and you want to add the ozonator to that.
Right. They’re actually two separate purchases. One is the water pick, and the second is the ozone machine. I actually put a website where you can actually buy it, but I encourage you to just go on the internet and look for one that has the characteristics that I’ve described.
I was just wondering about hydrogen peroxide. You said oxygen?
Not nearly as effective as the ozone. Ozone is O3, quite a bit more concentrated, and it actually kills bacteria a lot of more effectively. You don’t have to be purchasing hydrogen peroxide for the rest of your life. You just buy your machine once. I’ve had my ozone generator for about 25 years.
How do you make you own toothpaste?
I actually give the recipe to all my patients when they come in and get their propiece, but I have posted it in our blog. You know, what we’re going to do.
Next week, when we send you the link to the website to go to so that you can watch this for an entire month again, we’re going to include the link to his slide presentation for you and we might actually get his recipe to send to you.
Yeah. I can actually make it available to send to you guys, and it’s also in my blog. If you go to drvinograd.com, I have it there. I actually wrote an article about toothpastes, and if you want to see what they’re putting on your toothpaste, it’s like a Halloween story. It’s kind of scary.
Okay. So, we’re going to move on, and I’ll take some more questions at the end as well. The root canal controversy. This is the biggie. This is the mother of all questions, at least in my practice. I just had a lady contact me from Toronto, and she went to see a naturopathic doctor. She had eight root canals, and they wanted to extract the eight teeth.
So, you know you really have to start thinking. You really have to start using your head when you’re going to make a decision like this. Our root canal’s a problem. Do we leave it? Do we treat it? Do we extract it? What I was talking about before in the internet and getting a lot of information, there are patients that come to me and say, “Doc, I heard root canals are the greatest evil in this world. There’s just nothing worse than a root canal. I want you to take my tooth out.” Ultimately I will if I understand that the patient understands what they’re doing.
If they have all the facts and I can make a decision with him based on intelligent information because I’m not going to be making the decisions for them unless it’s something that I don’t feel comfortable doing that are going to impact their lives. I think you have to make the decisions that are going to impact your lives by having good information.
So, let’s talk about what a root canal is. Basically, the pulp, which is a combination of a nerve and some vessels, a vein and an artery, run through the inside of the tooth. Now, when there’s decay and the decay invades the nerve, that nerve becomes diseased. It becomes infected, and then, we have to decide what we’re going to do with it.
So, let’s go back. So, what do we do? In the past, people have gone in there. They’ve created a little perforation on the top of the tooth, go in there, remove the pulp, the nerve, and it really is a very painless procedure. It sounds awful, but it’s really a painless procedure, at least in our office, and then, you actually enlarge the canals a little bit, clean them out, disinfect them. Then, you fill them with material.
Now, in a perfect world, if you could fill them and seal them, you would have a viable situation. What has given root canals such a bad name is that 99% of all root canals being done today are being filled with gutta purcha which is a rubber with some sealant, like a paste, that hardens, and a few other pieces of rubber. Some of them use heat to melt their rubber.
Some dentists will actually condense it and push it to try to get some kind of mass to fill that area. All of that has been terribly inappropriate and insufficient to really create a proper seal. First of all, the sealers that have been very toxic, and secondly, by both of these methods, you cannot really get a good seal where you don’t have voids.
Now, those little voids, mini-voids that you get by doing a traditional root canal is what creates the problem because when you have those little voids they get invaded by bacteria, anaerobic bacteria, and there’s no way to get them once they get in there. How do you get them out? So, that has been the problem in the past.
People say you have a dead tooth and a lot of other things. Well, not totally. It’s a functional tooth. You still have blood supply from the outside. Do they get more brittle? Yes. Is that a perfect situation? No, but you have to understand. How is this going to impact your life?
My advice to this lady from Toronto that called me. I said, “You know, send me your x-rays. I’ll look at them.” I looked at the x-rays. There was one particular tooth that I felt was really not a good candidate for a root canal.
I said, “Why don’t you extract this tooth, have the dentist put some kind of organic material to maintain the bone quality just in case you want to change your mind later and put something in there so that you don’t lose your bone. Then, go for three months, and get a fill how it is to live without this tooth.”
Then, multiply that times however many teeth they want to take out and see what the quality of your life going to be? What is the quality of your life going to be with a removable denture? Our quality of life impacts our health, too. So, the decision to go black or white sometimes are not the best decisions. We have to really see how immune compromised we are, what the situation is, what the quality of life is going to be post-decision and so forth. So, again, just have good information to make your decisions.
So, options to replace extracted teeth. Let’s say you decide to get rid of the tooth. We could do an implant, and there a couple of different kinds of implants. There are implants made of titanium, and recently, from Europe, some dentists have been importing a new technology which they’re doing. They’re zirconium implants. I don’t do zirconium implants in my practice because I think they still have a lot of challenges. They’re still one piece. They’re very large. They’re very invasive. So, I don’t feel that they’re just where we need them to be yet.
You can use a fixed bridge to replace missing tooth. You can use a removable bridge or a Maryland Bridge. Here is an implant. What is an implant? It’s basically a piece of titanium that’s embedded on your bone, and a crown gets placed. Is that perfect? No. Is that something that you have to think about twice before doing? Of course.
Again, they integrate well into the bone, but it is a metal in your bone. There’s no way around it. People are going to try to sell you. “This is the right answer. This is good. This is bad.” There’s no good. There’s no bad. It’s what’s right for you.
11/13 Lecture: Holistic Dental Health (Transcribed) P3
Dentists exposed to the mercury get some damage, too?
Yes, absolutely. The reason I’m standing here today is because over 30 years ago, I felt really sick, and I was wondering, “Oh god, I’m in my 30s. This is what getting old must feel like.” I felt really lousy. I said, “Okay, I accept. I’m getting older.” Then, I realized that I was incredibly mercury toxic. So, I had a lot of memory problems, constant fatigue. So, this is how I really got started into becoming a naturopath and getting interested. So, yeah, especially dentists that continue to use amalgam are quite exposed, not so much now as we used to be because 35 years ago, we were not using gloves and masks and so forth, but, even today, when we remove the amalgams, we actually protect ourselves.
How many years do you think a dentist gets damaged with the mercury?
How many years?
How many years does it take for a mercury to damage a dentist? I’m telling this because my daughter’s a dentist. I don’t know if she’s doing the same with the thing like you are.
Yeah. Well, whatever she’s doing, whether she’s placing the amalgams or not, she’s probably is removing them all the time every day. So, she really should protect herself well against a lot of the fumes, a lot of the powders that are coming out. Definitely, it’s a great risk to her health. So, for you to intervene or give her some awareness would be an act of love and kindness.
Hello, doc. I have a question. It’s kind of a stretch, but is there any chance for people pulling their wisdom teeth, reusing some of their own material and growing your teeth back in some form, or using any form of material in your body like a bone of some sort that really can regrow itself and not have to use a foreign material outside your body?
Yeah, you know, in maybe 20, 30 years, but not at this point. Now, they are now developing tooth germs, where you can actually take the tooth out and place a tooth germ and grow it. That’s happening already. It’s just not happening fast enough because those germs take about seven to eight years to grow, and most of us don’t want go without a tooth for about seven to eight years. Stem cell? Yeah. All that is coming. All that is coming. Unfortunately, not here for us today yet.
Do you refer any of your clients who have had their amalgams removed before and not that way to a certain naturopath who can detox because I know I’ve had mine removed before, [and I still have some left. My doctor never thought they were a problem no matter how much I told him, and I would have pieces of it left in my mouth. He would suction it out, and I would swallow some. I know, and I know I’m feeling the effects of it every day, but is there a certain protocol?
So, your experience is not unique. This is the norm. This is what happens in dental offices all the time, not all of them. Yeah, a lot of the stuff that has gone systemic unfortunately the mercury gets lodged in the fatty tissues, and so they’re very, very hard to get rid of.
So, the first thing that you should do is maybe consult with a naturopath. I do work with naturopaths now, and they sometimes do some chelation, some testing, and so forth, but the first thing for you to do is to test yourself. There are different ways of doing it.
There’s a rough estimate of how you can do it with hair analysis. Then, there are other ways where you chelate and they test either your urine or feces to find out, but in order to do that, you have to dislodge a certain amount of the embedded toxins because if you just take a blood test they’re not going to appear because the toxin’s really embedded in the fatty tissues.
So, you have to take something like DMSA, DMTS, which is a little harsh. So, you don’t want to be doing this all the time. You want to do it with supervision to actually dislodge some of that from your fatty tissues into the bloodstream or into the urine or into the feces or fecal matter and test it. Once you know what you have, then, you can work with it because to detox, you also would need to know what it is you’re detoxing.
A lot of the heavy metals that are lower in the chart are more difficult to get rid of unless you get rid of some of the lighter heavy metals. So, there are protocols in which to do this. Okay. I’m going to continue, then, and we’re going to talk a little bit about oral disease and systemic disease. What’s interesting with a lot of the research that’s coming out lately is that they have found the same bacteria that you have in gum disease, in some decay, sometimes in root canals, that bacteria doesn’t stay in your mouth. It actually has access to the bloodstream. So, that bloodstream is actually carrying this bacteria to different parts of the body.
A lot of the really big problems is gum disease. This is something that you really need to be aware of because the gum disease actually is hosting a number of anaerobic bacteria, oxygen-hating bacteria in there. That’s why they hide inside the gums because they hate oxygen. So, they’re in there doing their thing. So, this is a more advanced case where you can see the gum disease, the inflammation, and there’s usually pockets right in between. So, you can see clearly. There’s a periodontal pocket. It’s the space between your tooth and your gum. That is a critical piece of information for you.
If you have two or three millimeters of space between your tooth and your gum, you can actually get in there and clean it with your toothbrush. If you start getting into four, five, six millimeters, now it starts becoming impossible to really clean this area with a toothbrush. So, up to here, I can go with a toothbrush. Down here, it’s untouchable. It’s bacteria right there as happy as could be. They’re throwing a party, 24/7. So, what’s happening with that? More inflammation, more bacteria, and our bone starts coming down, creating even more pocket depth.
So, this is one of the most critical things you can do for your health is to check to make sure that you don’t have deep pockets that are hosting a lot of anaerobic bacteria, oxygen-hating bacteria. Interesting that the same bacteria that have been found in some decays and some root canals, have been found in the heart of people that have been ill with heart disease, and in pancreatic research. There’s really some good, solid research done by some respected institutions that have found the same type of bacteria in the mouth and in some of these life-threatening diseases.
So, what do you do about periodontal disease? A lot of people have that. Some of us are aware of it. Some of us are not aware of that. Obviously, traditional is brushing, make sure that you use youth toothbrush, just a soft toothbrush with some water, and you actually introduce it into the pockets and clean them.
Then, after that, if you want to use toothpaste or whatever for your teeth, that’s fine, but you really should spend the time with water and a toothbrush physically removing. This is only going to remove the first two or three millimeters-worth of bacteria, right?
Now, this is something that I’ve actually been promoting for a long time. I thought I was the inventor of this, but when my son went to check this, [there were like 500 other people that had been using this irrigating device and also one form or the other. So, I guess I wasn’t so smart anymore, but this is some that I really work with my patients a lot and I really, highly recommend this as a much enhanced way to do your oral hygiene.
What you do is you actually purchase a water pick. You can purchase at any store. Any major store will carry them, Costco, Target. Any of them will have it, very, very moderately priced, and you start using the water pick. What the water pick will do is the water pick will actually access more than 3 millimeters. It will access the 4, 5, 6, and 7 millimeters if you actually get that water pick in between your tooth and your gum. So, now, we’re doing some physical removal of that bacteria.
Is this more important than going to see your dentist for gum disease? Don’t quote me on this, but yes. Why is this more important? Of course, it’s important to go every six months to get your pockets checked and get everything cleaned up. Of course, it’s important, but this you can do every day. I can’t come to your house. I would love to if you invite me, but you know. I can’t come to your house every day and clean your pockets out. You can. You are your best dentist.
Now, when you start introducing and ozonator, an ozone generator, it’s actually bubble the ozone into the container of your water pick. Using that water into your gums, now you’re taking O3, and hitting this anaerobic bacteria, which hate oxygen, which die on contact.
So, here, you have, without chemicals, without having to pay for a lot of expensive mouth rinses and medicated and chemically-filled washes, you can actually kill all the anaerobic bacteria that is causing all that disease. So, we found this of tremendous help.
In my own practice, I’ve kept a great number of patients from going into periodontal surgery, and they’re able to maintain it because, in essence, what does a periodontal surgeon do? They actually cut the pockets to make them 2 or 3 millimeters again so you can make them clean again so you can clean them. That’s basically what they do. I mean, they will also go in there and reshape the bone underneath, but really the bottom line is they’re just creating a situation where you can maintain it again without all these bacteria.
So, by using an ozone machine and a water pick, you’re enabling yourself, you’re empowering yourself to do this and keeping yourself from really having a lot of gum disease, which affects your body. So, some suggestions about the ozone. Use it in a well-ventilated area because ozone, in the air, is highly irritating to your GI tract, but in water it is perfectly safe.
The kind of ozonator that you want should have this specific specifications. It should be a corona discharge, preferably 1000 milligrams per hour because, otherwise, you’re going to be sitting there for two hours ozonating your water. With 1000 milligrams, you will actually ozonate your water in maybe 10 minutes. So, you just put it in there and go do something else. Ten minutes later, you come back, and you use your water with your water pick.
You want a sealed box around the elements. There are actually some people on the internet that are actually making their own machines. You know, I’m a little suspect of that. I actually had my son who has a company source this particular one. So, if you don’t find it anywhere else, you can always go to this website and get it. I’m not encouraging you to go buy it from him, if you find it somewhere else with those specs, I think you should get one. It’s wonderful for your whole family. I’ll let you read that yourselves.
Associate Dentist Wanted | San Diego, CA
Job Listing – San Diego Associate Dentist Position
We are looking for a gentle, motivated dentist with at minimum of two years experience, to join our successful, state of the art private practice.
We have an extraordinary, dynamic team, and are looking for a good match in philosophy, personality, and work ethic.
Required Skills:
- Able to produce quality dentistry on a very busy schedule.
- People oriented and team player, no drama.
If you are a recruiter or agency, please do not contact.
If you feel you may be a good match, please take a moment to learn a bit about us here, and from our practice website, San Diego Dentist – and call me at 619-630-7174. Resumes can also be sent to info@.
– Dr Daniel Vinograd, DDS.



 Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here:
Currently, I know that a number of you have been looking for ozonizers in order to follow my protocol (for prevention of gum disease). They can be found here: 
